

Exploratory study of tracheal extubation in operating room after single-lung transplantation
-
摘要:
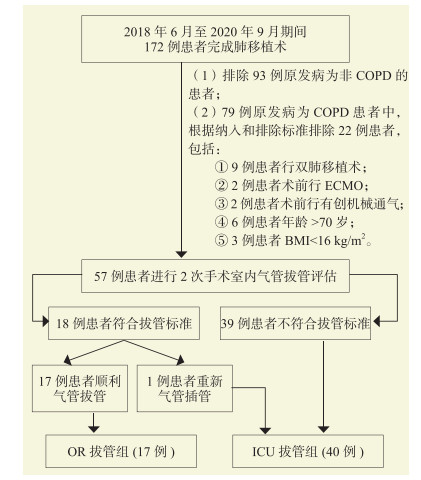
目的 探讨终末期慢性阻塞性肺疾病(COPD)患者单肺移植术后手术室内气管拔管方案的可行性及安全性。 方法 回顾性分析57例因终末期COPD行单肺移植的受者的临床资料,根据本院制定的手术室内气管拔管评估指标进行评估,符合条件、在手术室完成气管拔管的为手术室拔管组(OR拔管组,17例),在重症监护室(ICU)完成气管拔管的为ICU拔管组(40例)。比较两组术中气管拔管评估结果和术后康复情况。 结果 与ICU拔管组比较,OR拔管组受者的氧合指数较高,动脉血二氧化碳分压(PaCO2)、血乳酸水平较低,血压波动幅度较小,术中使用体外膜肺氧合(ECMO)的例数较少(均为P < 0.05)。OR拔管组2例受者分别于返回ICU 6、8 h再次气管插管,术后6、9 d拔除气管导管。OR拔管组受者术后机械通气时间、术后ICU入住时间、术后住院时间均较ICU拔管组受者短(均为P < 0.05)。两组受者术后原发性移植物功能障碍(PGD)3级、房性快速性心律失常、连续肾脏替代治疗例数和1年生存率比较,差异均无统计学意义(均为P > 0.05)。 结论 本院制定的COPD患者单肺移植术后手术室内气管拔管方案安全可行,可减少受者术后机械通气时间,缩短术后ICU入住时间及住院时间,不增加并发症发生率。 Abstract:Objective To evaluate the feasibility and safety of tracheal extubation in operating room for patients with end-stage chronic obstructive pulmonary disease (COPD) after single-lung transplantation. Methods Clinical data of 57 recipients who underwent single-lung transplantation due to end-stage COPD were retrospectively analyzed. According to the evaluation indexes of tracheal extubation in operating room established by our hospital, 17 recipients eligible for tracheal extubation in operating room were assigned into the operating room extubation group (OR extubation group) and 40 recipients receiving tracheal extubation in intensive care unit (ICU) were allocated in the ICU extubation group. The evaluation results of intraoperative tracheal extubation and postoperative recovery were compared between two groups. Results Compared with the ICU extubation group, recipients in the OR extubation group had higher oxygenation index, lower arterial partial pressure of carbon dioxide (PaCO2), lower blood lactic acid level, less fluctuation range of blood pressure and fewer cases receiving extracorporeal membrane oxygenation (ECMO) during operation (all P < 0.05). Two recipients in the OR extubation group received repeated tracheal intubation at 6 and 8 h after returning to ICU, and tracheal extubation at postoperative 6 and 9 d. In the OR extubation group, time of postoperative mechanical ventilation, length of postoperative ICU and hospital stay of the recipients were shorter than those in the ICU extubation group (all P < 0.05). The incidence of grade 3 primary graft dysfunction (PGD), atrial tachyarrhythmia, continuous renal replacement therapy and 1-year survival rate did not significantly differ between two groups (all P > 0.05). Conclusions The tracheal extubation regimen in the operating room for COPD patients after single-lung transplantation established by our hospital is safe and feasible, which shortens the time of postoperative mechanical ventilation, the length of postoperative ICU and hospital stay, whereas does not increase the incidence of postoperative complications. -
表 1 两组受者第2次手术室内气管拔管评估结果比较
Table 1. Comparsion of the assessment results of second extubation in the operating room of recipients between two groups
指标 OR拔管组(n=17) ICU拔管组(n=40) P值 氧合指数[M(P25,P75),mmHg] 287(240,379) 226(178,298) 0.004 PaCO2[M(P25,P75),mmHg] 43(38,47) 47(41,54) 0.026 血压波动幅度≤30%[n(%)] 17(100) 30(75) 0.025 出血量[M(P25,P75),mL] 200(100,400) 225(163,500) 0.700 尿量[M(P25,P75),mL] 750(600,1 200) 1 000(725,1 588) 0.175 血红蛋白[M(P25,P75),g/L] 122(111,129) 107(89,116) 0.112 血乳酸[M(P25,P75),mmol/L] 0.9(0.8,1.3) 1.5(1.2,2.0) 0.001 核心体温[M(P25,P75),℃] 36.8(36.7,37.0) 36.7(36.5,37.0) 0.265 术侧支气管吻合通畅[n(%)] 17(100) 40(100) 术侧气道血性分泌物 0.308 少量[n(%)] 17(100) 35(88) 中量[n(%)] 0 5(12) 术中使用ECMO[n(%)] 0 10(25) 0.025 mPAP[M(P25,P75),mmHg] 29(26,33) 31(26,37) 0.751 供肺冷缺血时间[M(P25,P75),min] 236(178,338) 240(200,410) 0.513  下载: 导出CSV
下载: 导出CSV
表 2 两组受者术后康复情况比较
Table 2. Comparison of postoperative recovery of recipients between two groups
指标 OR拔管组(n=17) ICU拔管组(n=40) P值 PGD 3级①[n(%)] 1(6) 12(30) 0.101 房性快速性心律失常[n(%)] 0 5(13) 0.308 术后机械通气时间[M(P25,P75),d] P1:6 P2:9② 4(2,8) < 0.001 连续肾脏替代治疗[n(%)] 0 6(15) 0.164 术后ICU入住时间[M(P25,P75),d] 5(5,7) 11(6,16) 0.002 术后住院时间[M(P25,P75),d] 15(12,24) 26(17,35) 0.009 1年生存率[n(%)] 16(94) 31(78) 0.259 注:①PGD 3级指氧合指数 < 200 mmHg,有与肺水肿一致的X线浸润表现[11]。
②由于病例数较少,在定量资料中以每例实际值表示,P1指病例1(patient 1),P2指病例2(patient 2)。
下载: 导出CSV
-
[1] MANDELL MS, HUANG J, ZHAO J. Enhanced recovery after surgery and practical application to liver transplantation[J]. Best Pract Res Clin Anaesthesiol, 2020, 34(1): 119-127. DOI: 10.1016/j.bpa.2020.02.001. [2] 易慧敏, 陆平兰. 加速康复外科在肝移植围手术期的应用[J]. 器官移植, 2020, 11(1): 41-46. DOI: 10.3969/j.issn.1674-7445.2020.01.006.YI HM, LU PL. Application of enhanced recovery after surgery in perioperative period of liver transplantation[J]. Organ Transplant, 2020, 11(1): 41-46. DOI: 10.3969/j.issn.1674-7445.2020.01.006. [3] LI J, WANG C, CHEN N, et al. Immediate postoperative tracheal extubation in a liver transplant recipient with encephalopathy and the Mayo end-stage liver disease score of 41: a CARE-compliant case report revealed meaningful challenge in recovery after surgery (ERAS) for liver transplantation[J]. Medicine (Baltimore), 2017, 96(47): e8467. DOI: 10.1097/MD.0000000000008467. [4] XU Q, ZHU M, LI Z, et al. Enhanced recovery after surgery protocols in patients undergoing liver transplantation: a retrospective comparative cohort study[J]. Int J Surg, 2020, 78: 108-112. DOI: 10.1016/j.ijsu.2020.03.081. [5] YAO YX, WU JT, ZHU WL, et al. Immediate extubation after heart transplantation in a child by remifentanil-based ultra-fast anesthesia: a case report[J]. Medicine (Baltimore), 2019, 98(5): e14348. DOI: 10.1097/MD.0000000000014348. [6] CRESPO MM, CLARIDGE T, DOMSIC RT, et al. ISHLT consensus document on lung transplantation in patients with connective tissue disease: part Ⅲ: pharmacology, medical and surgical management of post-transplant extrapulmonary conditions statements[J]. J Heart Lung Transplant, 2021, 40(11): 1279-1300. DOI: 10.1016/j.healun.2021.07.013. [7] CHEN F, CHIN K, SATO M, et al. Postoperative respiratory management in living donor lobar lung transplantation[J]. Clin Transplant, 2013, 27(4): E383-E390. DOI: 10.1111/ctr.12148. [8] ASSENZO V, ASSENZO C, FILIPPO R, et al. The feasibility of extubation in the operating room after bilateral lung transplantation in adult emphysema patients: an observational retrospective study[J]. Eur J Cardiothorac Surg, 2018, 54(6): 1128-1133. DOI: 10.1093/ejcts/ezy196. [9] AI Q, DENG H, HUANG D, et al. Early extubation in operating room after single-lung transplantation: a single institutional experience[J]. Ann Palliat Med, 2021, 10(4): 4134-4142. DOI: 10.21037/apm-20-1598. [10] 梁丽霞, 陈磊, 周延然, 等. 单肺移植术后手术室内气管拔管二例[J]. 临床麻醉学杂志, 2019, 35(11): 1143-1144. DOI: 10.12089/jca.2019.11.026.LIANG LX, CHEN L, ZHOU YR, et al. Two cases of extubation in operating room after single lung transplantation[J]. J Clin Anesthesiol, 2019, 35(11): 1143-1144. DOI: 10.12089/jca.2019.11.026. [11] CANTU E, DIAMOND JM, SUZUKI Y, et al. Quantitative evidence for revising the definition of primary graft dysfunction after lung transplant[J]. Am J Respir Crit Care Med, 2018, 197(2): 235-243. DOI: 10.1164/rccm.201706-1140OC. [12] 胡春晓, 李小杉, 卫栋, 等. 前进中的肺移植事业——我国肺移植发展现状及未来[J]. 器官移植, 2020, 11(2): 204-207. DOI: 10.3969/j.issn.1674-7445.2020.02.005.HU CX, LI XS, WEI D, et al. The development of lung transplantation: current situation and future of lung transplantation in China[J]. Organ Transplant, 2020, 11(2): 204-207. DOI: 10.3969/j.issn.1674-7445.2020.02.005. [13] YOUNG KA, DILLING DF. The future of lung transplantation[J]. Chest, 2019, 155(3): 465-473. DOI: 10.1016/j.chest.2018.08.1036. [14] 伍威, 邹捍东, 谢文杰, 等. 加速康复外科优化肺移植患者术后重症监护管理的经验[J]. 武汉大学学报(医学版), 2021, 42(4): 542-545. DOI: 10.14188/j.1671-8852.2021.6008.WU W, ZOU HD, XIE WJ, et al. Experience of ERAS in optimizing intensive care management after lung transplantation[J]. Med J Wuhan Univ, 2021, 42(4): 542-545. DOI: 10.14188/j.1671-8852.2021.6008. [15] FESSLER J, FISCHLER M, SAGE E, et al. Operating room extubation: a predictive factor for 1-year survival after double-lung transplantation[J]. J Heart Lung Transplant, 2021, 40(5): 334-342. DOI: 10.1016/j.healun.2021.01.1965. [16] FAEH D, KAUFMANN M, HAILE SR, et al. BMI-mortality association: shape independent of smoking status but different for chronic lung disease and lung cancer[J]. Int J Chron Obstruct Pulmon Dis, 2018, 13: 1851-1855. DOI: 10.2147/COPD.S157629. [17] KIM EK, SINGH D, PARK JH, et al. Impact of body mass index change on the prognosis of chronic obstructive pulmonary disease[J]. Respiration, 2020, 99(11): 943-953. DOI: 10.1159/000511022. [18] WILES SP, LANE CR, ATAYA A, et al. Non-invasive positive pressure ventilation in lung transplant recipients with acute respiratory failure: beyond the perioperative period[J]. J Crit Care, 2018, 47: 287-294. DOI: 10.1016/j.jcrc.2018.07.028. [19] KOTECHA S, BUCHAN C, PARKER K, et al. Domiciliary non-invasive ventilation post lung transplantation[J]. Respirology, 2018, 23(1): 96-99. DOI: 10.1111/resp.13160. [20] WADSWORTH LE, BELCHER J, BRIGHT-THOMAS RJ. Non-invasive ventilation is associated with long-term improvements in lung function and gas exchange in cystic fibrosis adults with hypercapnic respiratory failure[J]. J Cyst Fibros, 2021, 20(5): e40-e45. DOI: 10.1016/j.jcf.2021.05.011. [21] CHIUMELLO D, CHEVALLARD G, GREGORETTI C. Non-invasive ventilation in postoperative patients: a systematic review[J]. Intensive Care Med, 2011, 37(6): 918-929. DOI: 10.1007/s00134-011-2210-8. [22] GARRAMONE A, CANGEMI R, BRESCIANI E, et al. Early decrease of oxidative stress by non-invasive ventilation in patients with acute respiratory failure[J]. Intern Emerg Med, 2018, 13(2): 183-190. DOI: 10.1007/s11739-017-1750-5. [23] YEUNG J, COUPER K, RYAN EG, et al. Non-invasive ventilation as a strategy for weaning from invasive mechanical ventilation: a systematic review and Bayesian Meta-analysis[J]. Intensive Care Med, 2018, 44(12): 2192-2204. DOI: 10.1007/s00134-018-5434-z. [24] VASCHETTO R, PECERE A, PERKINS GD, et al. Effects of early extubation followed by noninvasive ventilation versus standard extubation on the duration of invasive mechanical ventilation in hypoxemic non-hypercapnic patients: a systematic review and individual patient data Meta-analysis of randomized controlled trials[J]. Crit Care, 2021, 25(1): 189. DOI: 10.1186/s13054-021-03595-5. [25] CASEY JD, VAUGHAN ER, LLOYD BD, et al. Protocolized post-extubation respiratory support to prevent reintubation: protocol and statistical analysis plan for a clinical trial[J]. BMJ Open, 2019, 9(8): e030476. DOI: 10.1136/bmjopen-2019-030476. [26] HANSEN LN, RAVN JB, YNDGAARD S. Early extubation after single-lung transplantation: analysis of the first 106 cases[J]. J Cardiothorac Vasc Anesth, 2003, 17(1): 36-39. DOI: 10.1053/jcan.2003.7. [27] BAIDYA DK, KHANNA P, MAITRA S. Analgesic efficacy and safety of thoracic paravertebral and epidural analgesia for thoracic surgery: a systematic review and Meta-analysis[J]. Interact Cardiovasc Thorac Surg, 2014, 18(5): 626-635. DOI: 10.1093/icvts/ivt551. [28] OKOYE NU, MAJEKODUNMI AA, ILORI IU. Analgesic and opioid sparing effects of preoperative thoracic paravertebral block: a double blind evaluation of 0.5% bupivacaine with adrenaline in patients scheduled for simple mastectomy[J]. Niger Postgrad Med J, 2021, 28(2): 102-107. DOI: 10.4103/npmj.npmj_460_21. [29] CHAKOS A, FERRET P, MUSTON B, et al. Ex-vivo lung perfusion versus standard protocol lung transplantation-mid-term survival and Meta-analysis[J]. Ann Cardiothorac Surg, 2020, 9(1): 1-9. DOI: 10.21037/acs.2020.01.02. [30] TAKA H, MIYOSHI K, KUROSAKI T, et al. Lung transplantation via cardiopulmonary bypass: excellent survival outcomes from extended criteria donors[J]. Gen Thorac Cardiovasc Surg, 2019, 67(7): 624-632. DOI: 10.1007/s11748-019-01067-w. [31] DE PERROT M, LIU M, WADDELL TK, et al. Ischemia-reperfusion-induced lung injury[J]. Am J Respir Crit Care Med, 2003, 167(4): 490-511. DOI: 10.1164/rccm.200207-670SO. -

 下载:
下载:

 点击查看大图
点击查看大图
图(2) / 表(2)
计量
- 文章访问数: 297
- HTML全文浏览量: 118
- PDF下载量: 85
- 被引次数: 0


