

-
摘要: 胰腺移植和胰肾联合移植是治疗1型糖尿病和部分2型糖尿病及其并发症导致的肾衰竭的最佳治疗方法。胰腺移植的类型主要包括同期胰肾联合移植(SPK)、肾移植后胰腺移植(PAK)和单纯胰腺移植(PTA)。在所有的胰腺移植类型中,对移植胰腺的活组织检查(活检)仍然是明确诊断其排斥反应并与其他并发症进行鉴别的最佳方法。本文对移植胰腺活检的方法及其相关的研究进展、移植胰腺活检排斥反应诊断标准及其进展、移植胰腺主要的并发症及其病理学表现进行阐述,旨在为指导临床对上述并发症予以准确诊断,良好地保障移植胰腺和受者的长期存活提供参考。Abstract: Pancreas transplantation and pancreas-kidney transplantation are the optimal treatment for renal failure caused by type 1 diabetes mellitus, partial type 2 diabetes mellitus and their complications. Pancreas transplantation mainly includes simultaneous pancreas-kidney transplantation (SPK), pancreas transplantation after kidney transplantation (PAK) and pancreas transplantation alone (PTA). Among all types of pancreas transplantation, biopsy of pancreas allograft remains the best method for definitively diagnosing rejection and differentiate it from other complications. In this article, biopsy methods of pancreas allograft and related research progress, diagnostic criteria and research progress on rejection of pancreas allograft biopsy, and main complications and pathological manifestations of pancreas allograft were illustrated, aiming to provide reference for guiding the clinical diagnosis of the above mentioned complications and ensuring the long-term survival of pancreas allografts and recipients.
-
Key words:
- Simultaneous pancreas-kidney transplantation (SPK) /
- Pancreas transplantation after kidney transplantation (PAK) /
- Pancreas transplantation alone (PTA) /
- Antibody-mediated rejection (AMR) /
- T cell-mediated rejection (TCMR) /
- Donor specific antibody (DSA) /
- Chronic transplant arteriopathy (CTA) /
- Posttransplant lymphoproliferative disease (PTLD)
-

图 1 移植胰腺动脉血栓栓塞的病理解剖学表现
注:图示移植胰腺动脉主干剖开可见管腔内血栓栓塞(箭头所示)。
Figure 1. Pathoanatomical findings of arterial thromboembolism in pancreas allograft

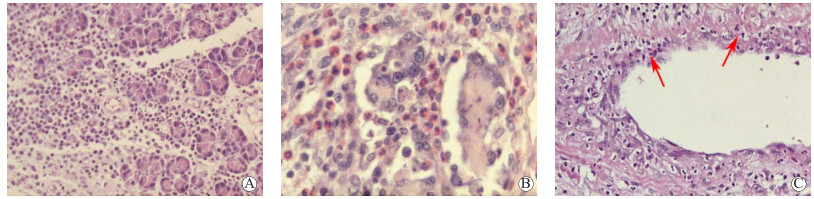
图 2 移植胰腺急性TCMR的腺泡及胰腺导管炎病变的病理学表现
注:A图示移植胰腺间质内大量的以淋巴细胞为主的单个核炎症细胞浸润(苏木素-伊红,×200);B图示胰腺间质内大量的单个核炎症细胞浸润并混合多数嗜酸性粒细胞浸润(苏木素-伊红,×400);C图示胰腺内导管上皮被淋巴细胞浸润形成导管上皮炎(箭头所示)(苏木素-伊红,×100)。
Figure 2. Pathological findings of acinar and pancreatic duct inflammatory lesions of acute TCMR in pancreas allograft

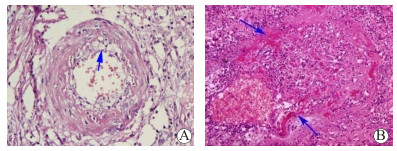
图 3 移植胰腺急性TCMR的血管病变的病理学表现
注:A图示动脉内膜淋巴细胞浸润及水肿致管腔轻度狭窄形成动脉内膜炎(箭头所示)(苏木素-伊红,×200);B图示动脉内膜大量淋巴细胞浸润和内膜水肿增厚及管壁平滑肌局部纤维素样坏死形成全层动脉炎(箭头所示)(苏木素-伊红,×200)。
Figure 3. Pathological findings of vascular lesions of acute TCMR in pancreas allograft

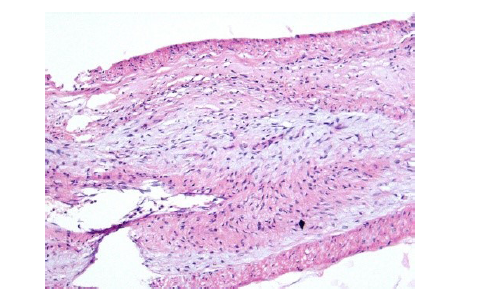
图 4 移植胰腺CTA的病理学表现
注:图示移植胰腺动脉分支内膜增生致管腔明显狭窄甚至闭塞(苏木素-伊红,×200)。
Figure 4. Pathological findings of CTA in pancreas allograft
表 1 2011年Banff移植胰腺排斥反应分级标准
Table 1. 2011 Banff schema for grading pancreas allograft rejection
分类 分级标准 正常 胰腺活检组织内无炎症细胞浸润,无动脉血管、胰腺导管异常,无任何胰腺腺泡损伤,胰腺小叶间隔规则 不确定的急性排斥反应 胰腺小叶间隔内可见极少许活化淋巴细胞浸润但不足以达到诊断轻度急性TCMR的标准 急性TCMR Ⅰ级(轻度):小叶间隔内活化的淋巴细胞浸润,有时可伴有嗜酸性粒细胞浸润,并常伴有下列病变中的一种,血管炎、和(或)胰腺导管炎、和(或)局灶性腺泡损伤或轻微坏死(胰腺小叶内 < 2个的局灶性炎症细胞浸润,但没有或仅有非常轻微的腺泡损伤)。Ⅱ级(中度):具有下列病变中的1项或2项,胰腺小叶内有≥3个的、多灶性的炎症细胞浸润,炎症浸润并未相互连接和呈弥漫性浸润,并有孤立的或散在的腺泡细胞因凋亡或坏死所致的脱失;轻微的血管内膜炎,表现为血管内皮少许单个核炎症细胞贴附浸润但没有内皮损伤所致的水肿表现。这一类型需要注意与急性AMR相鉴别。Ⅲ级(重度):严重的腺泡损伤,弥漫性的、混合性的炎症细胞浸润(包括中性粒细胞、嗜酸性粒细胞和淋巴细胞在内)并有多灶性的腺泡损伤坏死,和(或)中度至重度血管内膜炎,和(或)坏死性动脉血管炎,这一类型需要注意与急性AMR相鉴别 AMR (1)病理学表现:腺泡间隔炎症细胞浸润、毛细血管炎和腺泡损伤(腺泡细胞水肿、凋亡和坏死;血管炎可继发血栓形成);
(2)C4d染色阳性:腺泡间隔 > 5%的毛细血管内皮呈阳性;
(3)具有明确的血清供者特异性抗体;
急性AMR:具备上述3项中的3项;基本确定的AMR:具备上述3项中的2项;需要排除AMR:仅具备上述3项中的1项;慢性活动性AMR:具备本分级中的AMR和慢性排斥反应或移植胰腺纤维化病变,但没有急性TCMR病变急性AMR Ⅰ级(轻度):胰腺小叶及腺泡结构保存完好,但有轻度的单个核炎症细胞或混合性炎症细胞浸润和零星的腺泡细胞损伤的表现;Ⅱ级(中度):大部分腺泡小叶及腺泡结构保存完好,但有腺泡小叶间隔内可见单个核炎症细胞或混合性炎症细胞浸润,毛细血管扩张伴毛细血管炎,毛细血管淤血和出血,多灶性腺泡细胞坏死脱失;Ⅲ级(重度):不同程度的胰腺小叶及腺泡结构破坏及紊乱,动脉和静脉血栓形成及胰腺腺泡间质显著出血致多灶性或弥漫性胰腺组织坏死,以及相对稀疏的单个核炎症细胞和(或)中性粒细胞炎症浸润 慢性移植物动脉血管病 移植胰腺内动脉内膜纤维化增生、增厚,并在增生的内膜内有炎症细胞浸润 慢性排斥反应或移植胰腺纤维化 Ⅰ期(轻度纤维化):胰腺小叶纤维间隔增生增宽,纤维化组织的面积占活检胰腺组织面积 < 30%,少许胰腺小叶结构不规则;Ⅱ期(中度纤维化):纤维化组织的面积占活检胰腺组织面积30%~60%,多数腺泡萎缩导致胰腺组织结构不规则和腺泡被宽厚的纤维组织穿插和分割;Ⅲ期(重度纤维化):纤维化组织的面积占活检胰腺组织面积 > 60%,活检组织大部分均为纤维化组织,而残余的胰腺组织成为被分割的孤岛 胰岛病变 移植胰腺复发性糖尿病时出现胰岛炎和胰岛β细胞脱失 其他病理学改变 与急性和慢性排斥反应无关的病变,包括巨细胞病毒性胰腺炎、移植后淋巴组织增生性疾病等  下载: 导出CSV
下载: 导出CSV
-
[1] 郭晖. 胰腺移植病理学[M]//陈实, 郭晖. 移植病理学. 北京: 人民卫生出版社, 2009: 269-298. [2] 中华医学会器官移植学分会. 移植胰腺病理学临床操作规范(2019版)[J]. 器官移植, 2019, 10(6): 628-637. DOI: 10.3969/j.issn.1674-7445.2019.06.002.Branch of Organ Transplantation of Chinese Medical Association. Clinical operation specification for pancreas allograft pathology (2019 edition)[J]. Organ Transplant, 2019, 10(6): 628-637. DOI: 10.3969/j.issn.1674-7445.2019.06.002. [3] GUNTHER BROCKMANN J, BUTT A, ALHUSSAINI HF, et al. Protocol duodenal graft biopsies aid pancreas graft surveillance[J]. Transplantation, 2019, 103(3): 622-629. DOI: 10.1097/TP.0000000000002412. [4] PLANZ V, GALGANO SJ. Percutaneous biopsy and drainage of the pancreas[J]. Abdom Radiol (NY), 2021: 1-20. DOI: 10.1007/s00261-021-03244-z. [5] UVA PD, ODORICO JS, GIUNIPPERO A, et al. Laparoscopic biopsies in pancreas transplantation[J]. Am J Transplant, 2017, 17(8): 2173-2177. DOI: 10.1111/ajt.14259. [6] PATIL DT, YERIAN LM. Pancreas transplant: recent advances and spectrum of features in pancreas allograft pathology[J]. Adv Anat Pathol, 2010, 17(3): 202-208. DOI: 10.1097/PAP.0b013e3181d97635. [7] ARROYO ST, MARCANO LC, FERNÁNDEZ GT, et al. Pancreas-kidney transplantation: do we know the frequency of clinical complications?[J]. Transplant Proc, 2021, 53(9): 2692-2694. DOI: 10.1016/j.transproceed.2021.09.002. [8] GRUESSNER AC, GRUESSNER RW. P. 135: better long-term patient and kidney graft outcome for simultaneous pancreas/kidney (SPK) versus kidney transplant alone (KTA) recipients[J]. Transplantation, 2021, 105(12S1): S53. DOI: 10.1097/01.tp.0000804604.90540.9b. [9] RYU JH, KO HJ, SHIM JR, et al. Eosinophil-to-monocyte ratio is an excellent predictor of acute cellular rejection in pancreas transplant alone recipients[J]. Clin Transplant, 2020, 34(3): e13785. DOI: 10.1111/ctr.13785. [10] MAUPOEY IBÁÑEZ J, BOSCÀ ROBLEDO A, LÓPEZ-ANDUJAR R. Late complications of pancreas transplant[J]. World J Transplant, 2020, 10(12): 404-414. DOI: 10.5500/wjt.v10.i12.404. [11] UVA PD, PAPADIMITRIOU JC, DRACHENBERG CB, et al. Graft dysfunction in simultaneous pancreas kidney transplantation (SPK): results of concurrent kidney and pancreas allograft biopsies[J]. Am J Transplant, 2019, 19(2): 466-474. DOI: 10.1111/ajt.15012. [12] RYU JH, LEE TB, PARK YM, et al. Pancreas transplant with duodeno-duodenostomy and caval drainage using a diamond patch graft: a single-center experience[J]. Ann Transplant, 2017, 22: 24-34. DOI: 10.12659/aot.901469. [13] BÜTTNER-HEROLD M, AMANN K, PFISTER F, et al. Pancreas transplantation-clinic, technique, and histological assessment[J]. Pathologe, 2021, 42(5): 509-523. DOI: 10.1007/s00292-021-00982-1. [14] NORDHEIM E, HORNELAND R, AANDAHL EM, et al. Pancreas transplant rejection episodes are not revealed by biopsies of the donor duodenum in a prospective study with paired biopsies[J]. Am J Transplant, 2018, 18(5): 1256-1261. DOI: 10.1111/ajt.14658. [15] NAKHLEH RE, SUTHERLAND DE, BENEDETTI E, et al. Diagnostic utility and correlation of duodenal and pancreas biopsy tissue in pancreaticoduodenal transplants with emphasis on therapeutic use[J]. Transplant Proc, 1995, 27(1): 1327-1328. http://www.ncbi.nlm.nih.gov/pubmed/7878902 [16] KLASSEN DK, WEIR MR, CANGRO CB, et al. Pancreas allograft biopsy: safety of percutaneous biopsy-results of a large experience[J]. Transplantation, 2002, 73(4): 553-555. DOI: 10.1097/00007890-200202270-00011. [17] NAKHLEH RE, SUTHERLAND DE. Pancreas rejection. significance of histopathologic findings with implications for classification of rejection[J]. Am J Surg Pathol, 1992, 16(11): 1098-1107. http://www.ncbi.nlm.nih.gov/pubmed/1471730 [18] DRACHENBERG CB, PAPADIMITRIOU JC, KLASSEN DK, et al. Evaluation of pancreas transplant needle biopsy: reproducibility and revision of histologic grading system[J]. Transplantation, 1997, 63(11): 1579-1586. DOI: 10.1097/00007890-199706150-00007. [19] DRACHENBERG CB, ODORICO J, DEMETRIS AJ, et al. Banff schema for grading pancreas allograft rejection: working proposal by a multi-disciplinary international consensus panel[J]. Am J Transplant, 2008, 8(6): 1237-1249. DOI: 10.1111/j.1600-6143.2008.02212.x. [20] DRACHENBERG CB, TORREALBA JR, NANKIVELL BJ, et al. Guidelines for the diagnosis of antibody-mediated rejection in pancreas allografts-updated Banff grading schema[J]. Am J Transplant, 2011, 11(9): 1792-1802. DOI: 10.1111/j.1600-6143.2011.03670.x. [21] TATAPUDI VS, KOPCHALⅡSKA D, DA GENTE GJ, et al. Solid-phase C1q/C3d fixing readouts correlate with high median fluorescence intensity (MFI) de novo donor-specific HLA antibodies and C4d+ antibody-mediated rejection in kidney transplant recipients[J]. Ann Transplant, 2021, 26: e934175. DOI: 10.12659/AOT.934175. [22] ROUFOSSE C, DRACHENBERG C, RENAUDIN K, et al. Molecular assessment of antibody-mediated rejection in human pancreas allograft biopsies[J]. Clin Transplant, 2020, 34(11): e14065. DOI: 10.1111/ctr.14065. [23] TORREALBA JR, SAMANIEGO M, PASCUAL J, et al. C4d-positive interacinar capillaries correlates with donor-specific antibody-mediated rejection in pancreas allografts[J]. Transplantation, 2008, 86(12): 1849-1856. DOI: 10.1097/TP.0b013e3181902319. [24] NAKAMURA T, SHIROUZU T. Antibody-mediated rejection and recurrent primary disease: two main obstacles in abdominal kidney, liver, and pancreas transplants[J]. J Clin Med, 2021, 10(22): 5417. DOI: 10.3390/jcm10225417. [25] HAAS M. Evolving criteria for the diagnosis of antibody-mediated rejection in renal allografts[J]. Curr Opin Nephrol Hypertens, 2018, 27(3): 137-143. DOI: 10.1097/MNH.0000000000000398. [26] LOUPY A, HAAS M, SOLEZ K, et al. The Banff 2015 kidney meeting report: current challenges in rejection classification and prospects for adopting molecular pathology[J]. Am J Transplant, 2017, 17(1): 28-41. DOI: 10.1111/ajt.14107. [27] BRUGGEMAN BS, CAMPBELL-THOMPSON M, FILIPP SL, et al. Substance use affects type 1 diabetes pancreas pathology: implications for future studies[J]. Front Endocrinol (Lausanne), 2021, 12: 778912. DOI: 10.3389/fendo.2021.778912. [28] RAMIREZ DG, CICCAGLIONE M, UPADHYAY AK, et al. Detecting insulitis in type 1 diabetes with ultrasound phase-change contrast agents[J]. Proc Natl Acad Sci U S A, 2021, 118(41): e2022523118. DOI: 10.1073/pnas.2022523118. [29] NAYAGAM JS, HENEGHAN MA, SAMYN M, et al. Epstein-Barr virus status and immunosuppression use in paediatric autoimmune liver disease[J]. Aliment Pharmacol Ther, 2021, 55(4): 455-463. DOI: 10.1111/apt.16708. [30] SAMANT H, VAITLA P, KOTHADIA JP. Post transplant lymphoproliferative disorders[M]. Treasure Island (FL): StatPearls Publishing, 2022. -

 下载:
下载:



 点击查看大图
点击查看大图
计量
- 文章访问数: 353
- HTML全文浏览量: 110
- PDF下载量: 86
- 被引次数: 0


