

Clinical analysis of severe community-acquired pneumonia complicated with mediastinal emphysema after renal transplantation (report of 9 cases)
-
摘要:
目的 探讨肾移植术后重症社区获得性肺炎(CAP)合并纵隔气肿的临床治疗和转归。 方法 回顾性分析9例肾移植术后重症CAP合并纵隔气肿患者的临床资料。记录患者入重症监护室(ICU)时的急性生理学及慢性健康状况评分Ⅱ(APACHEⅡ)及氧合指数。观察患者的纵隔气肿合并症情况及相应的处理,记录患者在ICU期间的治疗经过、ICU病死率、ICU住院时间、总住院时间。所有患者行病原学检查。 结果 9例肾移植术后重症CAP合并纵隔气肿患者的APACHEⅡ评分为14(8~21)分,氧合指数为150(133~189)mmHg。9例患者中,单纯细菌感染3例;细菌感染合并病毒感染3例;结核分枝杆菌合并其他细菌感染1例;病毒感染1例;1例患者未找到病原学证据。纵隔气肿并发皮下气肿7例,并发气胸6例。治疗方式包括抗感染,调整免疫抑制方案,纵隔引流、胸腔闭式引流、皮下切开及体外膜肺氧合(ECMO)治疗。6例患者行有创正压通气(IMV), 2例行无创正压通气(NIV),1例经鼻高流量吸氧(HFNC)。9例患者中,ICU病死率为6/9,其余3例患者均恢复出院,ICU住院时间26(17~40)d,总住院时间27~61 d。 结论 纵隔气肿是肾移植术后重症CAP的严重并发症,病死率高。对此类患者应加强影像学评估、及时引流、充分镇静,必要时行ECMO治疗。 Abstract:Objective To investigate the clinical treatment and outcomes of severe community-acquired pneumonia (CAP) complicated with mediastinal emphysema after renal transplantation. Methods Clinical data of9 patients with severe CAP complicated with mediastinal emphysema after renal transplantation were retrospectively analyzed. The acute physiology and chronic health evaluationⅡ(APACHEⅡ) and oxygenation index were recorded when the patients were admitted to the intensive care unit (ICU). The complications of mediastinal emphysema and corresponding treatment were observed. The treatment course during the ICU, mortality rate in ICU, ICU stay time and hospital stay time were recorded. All patients underwent pathogenic examinations. Results The APACHEⅡ score of9 patients with severe CAP complicated with mediastinal emphysema after renal transplantation was 14 (8-21) scores and the oxygenation index was 150 (133-189) mmHg. Among 9 patients, 3 cases were infected by bacteria alone, 3 cases were infected by bacterial infection combined with viral infection, 1 case was infected by mycobacterium tuberculosis complicated with other bacterial infection and 1 case was viral infection. No pathogenic evidence was detected in the remaining 1 patient. Mediastinal emphysema complicated with subcutaneous emphysema occurred in 7 cases and pneumothorax occurred in 6 cases. Treatment methods included anti-infection, modified immunosuppressive program, mediastinal drainage, thoracic closed drainage, subcutaneous incision and extracorporeal membrane oxygenation (ECMO) treatment. Six patients received invasive mechanical ventilation (IMV), 2 received non-invasive positive pressure ventilation (NIV) and 1 received high-flow nasal oxygen cannula (HFNC). Among 9 patients, the mortality rate in ICU was 6/9, the remaining 3 patients were recovered and discharged, the ICU stay time was 26 (17-40) d, and the total hospital stay time was 27-61 d. Conclusions Mediastinal emphysema is a serious complication of patients presenting with severe CAP after renal transplantation with a high mortality rate. For these patients, imaging evaluation, timely drainage and full sedation should be strengthened, and ECMO treatment should be delivered when necessary. -

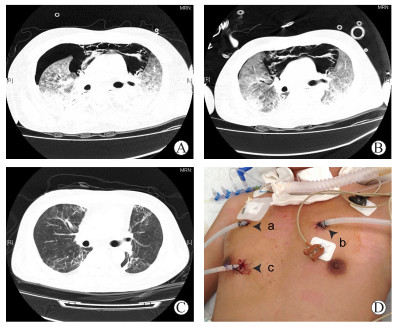
图 1 1例肾移植术后重症CAP合并纵隔气肿并发气胸的CT扫描和引流情况
A~C图为患者的CT扫描;D图为患者分别放置的右侧胸腔引流管(a)、左侧胸腔引流管(b)和纵隔引流管(c)
Figure 1. CT scans and drainages of 1 case with severe CAP complicated with pneumomediastinum and pneumothorax after renal transplantation
表 1 9例肾移植术后重症CAP合并纵隔气肿的临床资料
Table 1. Clinical data of 9 cases with severe CAP complicated with pneumomediastinum after renal transplantation
例序 年龄(岁) 性别 原发病 既往肺部疾病 移植后时间(月) CAP后出现纵隔气肿时间(d) 初始免疫抑制方案 1 55 女 肾小球肾炎 无 2 5 FK506+MMF+Pred 2 55 男 未确定 无 1 14 CsA+MMF+Pred 3 58 男 未确定 无 7 9 CsA+MMF+Pred 4 29 男 未确定 无 9 5 CsA+MMF+Pred 5 62 男 未确定 无 2 3 FK506+MMF+Pred 6 73 女 膜性肾病 无 89 52 CsA+MMF+Pred 7 30 男 IgA肾病 无 2 5 FK506+MMF+Pred 8 41 男 未确定 无 2 2 FK506+MMF+Pred 9 30 男 膜性肾病 无 7 17 FK506+MMF+Pred CsA为环孢素, FK506为他克莫司, MMF为吗替麦考酚酯, Pred为泼尼松  下载: 导出CSV
下载: 导出CSV
表 2 9例肾移植术后重症CAP合并纵隔气肿的情况和处理方法
Table 2. Situation and treatment of 9 cases with severe CAP complicated with pneumomediastinum after renal transplantation
例序 年龄(岁) 性别 氧疗方式 纵隔气肿合并情况 纵隔气肿处理 1 55 女 NIV 气胸+纵隔气肿+皮下气肿 纵隔引流+胸腔闭式引流 2 55 男 IMV 气胸+纵隔气肿+皮下气肿 纵隔引流+胸腔闭式引流 3 58 男 IMV 气胸+纵隔气肿+皮下气肿 纵隔引流+胸腔闭式引流 4 29 男 HFNC 纵隔气肿 未引流 5 62 男 IMV 气胸+纵隔气肿+皮下气肿 皮下切开+胸腔闭式引流+ECMO 6 73 女 IMV 纵隔气肿+皮下气肿 皮下切开 7 30 男 IMV 纵隔气肿+皮下气肿 皮下切开+纵隔引流+胸腔闭式引流 8 41 男 IMV 气胸+纵隔气肿+皮下气肿 胸腔闭式引流 9 30 男 NIV 气胸+纵隔气肿 胸腔闭式引流
下载: 导出CSV
-
[1] DIZDAR OS, ERSOY A, AKALIN H.Pneumonia after kidney transplant:incidence, risk factors, and mortality[J]. Exp Clin Transplant, 2014, 12(3):205-211. http://d.old.wanfangdata.com.cn/NSTLQK/NSTL_QKJJ0222031385/ [2] CANET E, OSMAN D, LAMBERT J, et al.Acute respiratory failure in kidney transplant recipients:a multicenter study[J]. Crit Care, 2011, 15(2):R91.DOI: 10.1186/cc10091. [3] IYER VN, JOSHI AY, RYU JH.Spontaneous pneumomediastinum:analysis of 62 consecutive adult patients[J]. Mayo Clin Proc, 2009, 84(5):417-421.DOI: 10.1016/S0025-6196(11)60560-0. [4] KIS A, SUTTO Z, TAMASI L, et al.Spontaneous pneumomediastinum after kidney transplantation:case report[J]. Transplant Proc, 2010, 42(6):2350-2352.DOI: 10.1016/j.transproceed.2010.05.016. [5] KERNS ES, ALOBAIDI SA, ROAYAIE K, et al.Chest pain after kidney transplantation owing to pneumomediastinum:a case report[J]. Transplant Proc, 2013, 45(7):2811-2814.DOI: 10.1016/j.transproceed.2013.02.143. [6] 中华医学会呼吸病学分会.中国成人社区获得性肺炎诊断和治疗指南(2016年版)[J].中华结核和呼吸杂志, 2016, 39(4):253-279.DOI: 10.3760/cma.j.issn.1001-0939.2016.04.005.Branch of Respiratory Medicine of Chinese Medical Association.Diagnosis and treatment guidelines of community acquired pneumonia in Chinese adults (2016 edition)[J]. Chin J Tubercu Respir Dis, 2016, 39(4):253-279.DOI: 10.3760/cma.j.issn.1001-0939.2016.04.005. [7] PADHY AK, GUPTA A, AIYER P, et al.Spontaneous pneumomediastinum:a complication of swine flu[J]. Asian Cardiovasc Thorac Ann, 2015, 23(8):998-1000.DOI: 10.1177/0218492315585907. [8] CHENG WL, KO WC, LEE NY, et al.Pneumomediastinum in patients with AIDS:a case report and literature review[J]. Int J Infect Dis, 2014, 22:31-34.DOI: 10.1016/j.ijid.2013.12.009. [9] MEIRA DIAS O, CAVALCANTI COELHO DL, RIBEIRO DE CARVALHO CR.Interstitial emphysema leading to pneumomediastinum in a bone marrow transplant patient[J]. Am J Respir Crit Care Med, 2013, 188(3):e4.DOI: 10.1164/rccm.201203-0385IM. [10] CANET E, ZAFRANI L, AZOULAY É.The critically Ⅲ kidney transplant recipient:a narrative review[J]. Chest, 2016, 149(6):1546-1555.DOI: 10.1016/j.chest.2016.01.002. [11] AZOULAY E, PICKKERS P, SOARES M, et al.Acute hypoxemic respiratory failure in immunocompromised patients:the Efraim multinational prospective cohort study[J]. Intensive Care Med, 2017, 43(12):1808-1819.DOI: 10.1007/s00134-017-4947-1. [12] ANZUETO A, FRUTOS-VIVAR F, ESTEBAN A, et al.Incidence, risk factors and outcome of barotrauma in mechanically ventilated patients[J]. Intensive Care Med, 2004, 30(4):612-619. doi: 10.1007/s00134-004-2187-7 [13] BROWER RG, LANKEN PN, MACINTYRE N, et al.Higher versus lower positive end-expiratory pressures in patients with the acute respiratory distress syndrome[J]. N Engl J Med, 2004, 351(4):327-336. doi: 10.1056/NEJMoa032193 [14] GALBOIS A, AIT-OUFELLA H, BAUDEL JL, et al.Pleural ultrasound compared with chest radiographic detection of pneumothorax resolution after drainage[J]. Chest, 2010, 138(3):648-655.DOI: 10.1378/chest.09-2224. [15] 朱洪章, 冯玉, 杨有优, 等.计算机辅助检测系统在数字化X线胸片肺结节筛查的临床应用[J].中山大学学报(医学科学版), 2017, 38(4):614-617. http://d.old.wanfangdata.com.cn/Periodical/zsykdxxb201704022ZHU HZ, FENG Y, YANG YY, et al.Clinical application of computer-aided detection system for pulmonary nodules on digital chest radiography[J]. J Sun Yat-sen Univ (Med Sci), 2017, 38(4):614-617. http://d.old.wanfangdata.com.cn/Periodical/zsykdxxb201704022 [16] TSCHOPP JM, BINTCLIFFE O, ASTOUL P, et al.ERS task force statement:diagnosis and treatment of primary spontaneous pneumothorax[J]. Eur Respir J, 2015, 46(2):321-335.DOI: 10.1183/09031936.00219214. [17] TU G, HE H, YIN K, et al.High-flow nasal cannula versus noninvasive ventilation for treatment of acute hypoxemic respiratory failure in renal transplant recipients[J]. Transplant Proc, 2017, 49(6):1325-1330.DOI: 10.1016/j.transproceed.2017.03.088. [18] PAPAZIAN L, FOREL JM, GACOUIN A, et al.Neuromuscular blockers in early acute respiratory distress syndrome[J]. N Engl J Med, 2010, 363(12):1107-1116.DOI: 10.1056/NEJMoa1005372. [19] YOUNG D, HARRISON DA, CUTHBERTSON BH, et al.Effect of early vs late tracheostomy placement on survival in patients receiving mechanical ventilation:the TracMan randomized trial[J]. JAMA, 2013, 309(20):2121-2129.DOI: 10.1001/jama.2013.5154. [20] FREEMAN BD, MORRIS PE.Tracheostomy practice in adults with acute respiratory failure[J]. Crit Care Med, 2012, 40(10):2890-2896. doi: 10.1097/CCM.0b013e31825bc948 [21] BRODIE D, BACCHETTA M.Extracorporeal membrane oxygenation for ARDS in adults[J]. N Engl J Med, 2011, 365(20):1905-1914.DOI: 10.1056/NEJMct1103720. -

 下载:
下载:

 点击查看大图
点击查看大图
计量
- 文章访问数: 140
- HTML全文浏览量: 77
- PDF下载量: 10
- 被引次数: 0


