

Experience of clinical efficacy of renal transplantation from donors of donation after brain death complicated with acute kidney injury
-
摘要:
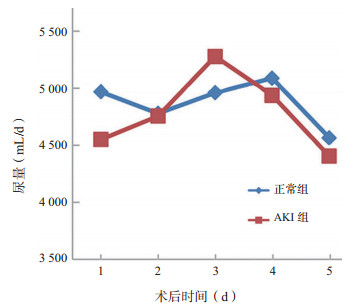
目的 总结伴急性肾损伤(AKI)的脑死亡器官捐献(DBD)供者供肾移植的治疗效果。 方法 选取成功完成DBD供肾移植的59例供者纳入本研究,根据入重症监护室(ICU)时的血清肌酐(Scr)水平,将DBD供者分为AKI组(14例)与正常组(45例),相应的101例受者根据供者情况分为AKI组(23例)与正常组(78例)。总结59例供者器官捐献情况,比较两组供者获取前的主要指标。比较两组受者术后肾功能、住院情况及临床结局。 结果 59例供者中,14例发生AKI(24%),其中2例在其维护期间行持续性肾脏替代治疗。与正常组供者相比,AKI组供者的急性生理与慢性健康(APACHE)Ⅱ评分明显升高(P<0.05),中枢性尿崩症的发生率更高(P<0.01),入ICU时和获取前的Scr水平更高(均为P<0.01),获取前24 h尿量更少(P<0.01)。与正常组受者相比,AKI组受者术后2、3 d的Scr水平更高(均为P<0.05),住院时间和住院花费亦明显升高(P<0.01,P<0.05)。两组受者术后移植肾功能延迟恢复、急性排斥反应、感染、恢复透析的发生率比较,差异无统计学意义(均为P>0.05)。术后3个月,两组受者均好转出院,移植肾存活率为100%。 结论 伴AKI的DBD供者供肾移植,经过积极的器官维护可纠正AKI,达到与非AKI供肾同样的效果,可以作为扩大供肾来源的途径。 Abstract:Objective To summarize the clinical efficacy of renal transplantation from donors of donation after brain death (DBD) complicated with acute kidney injury (AKI). Methods Fifty-nine DBD donors successfully undergoing renal transplantation were recruited in this investigation. According to the Scr level upon admission of intensive care unit (ICU), DBD donors were divided into the AKI group (n=14) and control group (n=45). A total of 101 recipients were assigned into the AKI group (n=23) and control group (n=78) correspondingly. The organ donation conditions of 59 donors were summarized. Main parameters of the donors before organ procurement were statistically compared between two groups. Postoperative kidney function, hospitalization condition and clinical outcomes of the recipients were statistically compared between two groups. Results Among 59 donors, 14 cases (24%) suffered from AKI. Two donors received continuous renal replacement therapy during organ maintenance. Compared with the donors in the control group, the APACHE Ⅱ score of the donors was significantly higher (P < 0.05), the incidence of central diabetes insipidus was considerably higher (P < 0.01), the Scr levels at admission of ICU and before organ procurement were significantly higher (both P < 0.01) and the amount of urine at 24 h before organ procurement was dramatically less in the AKI group (P < 0.01). Compared with the recipients in the control group, the Scr levels at postoperative 2 and 3 d were significantly higher (both P < 0.05), the length of hospital stay was considerably longer (P < 0.01) and the hospitalization expanse was significantly higher in the AKI group (P < 0.05). No statistical significance was observed in the postoperative delayed recovery of renal graft function, incidence of acute rejection, infection and rehabilitation dialysis in the recipients between two groups (all P > 0.05). At 3 months after transplantation, the recipients in two groups were discharged and the graft survival rate was 100%. Conclusions For renal transplantation from DBD donors complicated with AKI, active measures should be taken to maintain the organ and relieve the AKI, which yields similar clinical efficacy to renal transplantation from non-AKI donors and widens the origin of kidney graft. -

图 1 两组受者术后Scr水平的变化
Figure 1. Changes of Scr levels of recipients in two groups after operation

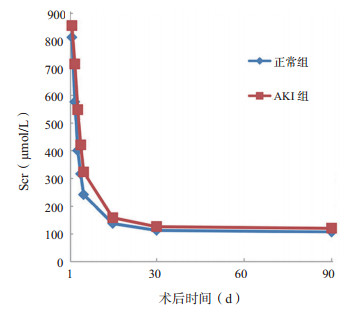
图 2 两组受者术后尿量的变化
Figure 2. Changes of urinary volume of recipients in two groups after operation
表 1 两组供者器官获取前主要指标的比较
Table 1. Comparision of the main indices of the donors between two groups before organ procurement
指标 AKI组(n=14) 正常组(n=45) 统计值 P值 APACHE Ⅱ评分(x±s,分) 22±6 18±50 2.677 0.010 发病至器官获取时间(x±s,d) 08(1~9) 06(1~10) -0.085 0.771 低血压[n(%)] 10(71) 21(47) -2.626 0.105 中枢性尿崩症[n(%)] 11(79) 17(38) 7.13 0.008 多巴胺剂量[M(R),µg/(kg·d)] 7.8(2.0~13.5) 5.0(0~8.5) -0.062 0.534 入ICU后血清钠离子水平最高值(x±s,mmol/L) 158±11 148±130 -0.816 0.370 获取前血清钠离子水平(x±s,mmol/L) 145±80 139±800 -0.001 0.972 入ICU时Scr水平(x±s,µmol/L) 0242±105 76±28 21.546 0.000 获取前Scr水平(x±s,µmol/L) 123±49 55±20 24.208 0.000 获取前24 h尿量[M(R),L] 0.9(0.3~2.5)0 1.9(0.4~2.8)0 -0.157 0.125  下载: 导出CSV
下载: 导出CSV
表 2 两组受者术后并发症发生率的比较
Table 2. Comparision of postoperative complication incidences of recipients between two groups
[n(%)] 指标 AKI组(n=23) 正常组(n=78) χ2值 P值 移植肾功能延迟恢复 9(39) 24(31) 0.564 0.452 急性排斥反应 16(70) 57(73) 0.109 0.741 感染 3(13) 7(9) 0.031 0.860 恢复透析 3(13) 08(10) 0.142 0.706
下载: 导出CSV
-
[1] Dhanani S, Shemie SD. Advancing the science of organ donor management[J]. Crit Care, 2014, 18(6): 612. DOI: 10.1186/s13054-014-0612-z. [2] 卫生部脑死亡判定标准起草小组.脑死亡判定标准(成人)(修订稿)[J].中国脑血管病杂志, 2009, 6(4): 220-224. DOI: 10.3969/j.issn.1672-5921.2009.04.014.The Drafting Group for Brain Death Criteria of Ministry of Health of the People's Republic of China. Judgement standard of brain death (for adult) (revised edition)[J]. Chin J Cerebrovasc Dis, 2009, 6(4): 220-224. DOI: 10.3969/j.issn.1672-5921.2009.04.014. [3] 急性肾损伤专家共识小组.急性肾损伤诊断与分类专家共识[J].中华肾脏病杂志, 2006, 22(11): 661-663.DOI: 10.3760/j.issn:1001-7097.2006.11.005.General Understanding Experts Group of Acute Kidney Injury. General understanding on the diagnosis and classification of acute kidney injury[J]. Chin J Nephrol, 2006, 22(11): 661-663. DOI: 10.3760/j.issn:1001-7097.2006.11.005. [4] Westphal GA, Garcia VD, Souza RL, et al. Guidelines for the assessment and acceptance of potential brain-dead organ donors[J]. Rev Bras Ter Intensiva, 2016, 28(3): 220-255. DOI: 10.5935/0103-507X.20160049. [5] Hall IE, Schröppel B, Doshi MD, et al. Associations of deceased donor kidney injury with kidney discard and function after transplantation[J]. Am J Transplant, 2015, 15(6): 1623-1631. DOI: 10.1111/ajt.13144. [6] Hahnenkamp K, Bohler K, Wolters H, et al. Organ-protective intensive care in organ donors[J]. Dtsch Arztebl Int, 2016, 113(33/34): 552-558. DOI: 10.3238/arztebl.2016.0552. [7] Ellis MK, Sally MB, Malinoski D. The development and current status of intensive care unit management of prospective organ donors[J]. India J Urol, 2016, 32(3): 178-185. DOI: 10.4103/0970-1591.185103. [8] Wan Q, Liu H, Ye S, et al. Confirmed transmission of bacterial or fungal infection to kidney transplant recipients from donated after cardiac death (DCD) donors in China: a single-center analysis[J]. Med Sci Monit, 2017, 23: 3770-3779. DOI: 10.12659/MSM.901884. [9] Matos AC, Requiao-Moura LR, Clarizia G, et al. Expanding the pool of kidney donors: use of kidneys with acute renal dysfunction[J]. Einstein(Sao Paulo), 2015, 13(2): 319-325. DOI: 10.1590/S1679-45082015RW3147. [10] Lee MH, Jeong EG, Chang JY, et al. Clinical outcome of kidney transplantation from deceased donors with acute kidney injury network criteria[J]. J Crit Care, 2014, 29(3): 432-437. DOI: 10.1016/j.jcrc.2013.12.016. [11] Farney AC, Rogers J, Orlando G, et al. Evolving experience using kidneys from deceased donors with terminal acute kidney injury[J]. J Am Coll Surg, 2013, 216(4): 645-656. DOI: 10.1016/j.jamcollsurg.2012.12.020. [12] Burker EJ, Fingerhut D, Ebneter D, et al. Emergency medical services knowledge and attitudes about non-heart-beating donors: effect of an educational intervention[J]. J Heart Lung Transplant, 2015, 34(2): 204-212. DOI: 10.1016/j.healun.2014.09.020. [13] 袁小鹏, 王长希, 周健, 等.伴急性肾功能衰竭的脑死亡器官捐献供者供肾移植26例报告[J].中华器官移植杂志, 2014, 35(12): 711-714. DOI: 10.3760/cma.j.issn.0254-1785.2014.12.002.Yuan XP, Wang CX, Zhou J, et al. Kidney transplantation from brain death donors with terminal acute renal failure: a report of 26 cases[J]. Chin J Organ Transplant, 2014, 35(12): 711-714. DOI: 10.3760/cma.j.issn.0254-1785.2014.12.002. [14] Pandit RA, Zirpe KG, Gurav SK, et al. Management of potential organ donor: Indian Society of Critical Care Medicine:position statement[J]. Indian J Crit Care Med, 2017, 21(5): 303-316. DOI: 10.4103/ijccm.IJCCM_160_17. [15] Yang SS, Yang J, Ahn C, et al. The need for new donor stratification to predict graft survival in deceased donor kidney transplantation[J]. Yonsei Med J, 2017, 58(3): 626-630. DOI: 10.3349/ymj.2017.58.3.626. [16] Jr CS, Koval CE, van Duin D, et al. Selecting suitable solid organ transplant donors: reducing the risk of donor-transmitted infections[J]. World J Transplant, 2014, 4(2): 43-56. DOI: 10.5500/wjt.v4.i2.43. -

 下载:
下载:

 点击查看大图
点击查看大图
计量
- 文章访问数: 127
- HTML全文浏览量: 52
- PDF下载量: 5
- 被引次数: 0


