

Analysis and management of critical value in renal transplantation recipients during perioperative period
-
摘要:
目的 分析并总结肾移植受者围手术期常见危急值的特点及处理方法。 方法 收集出现危急值的273例次肾移植围手术期患者的性别、年龄、危急值、原发病、出现危急值时临床诊断及相应处理等资料并进行分析。 结果与结论 肾移植受者在围手术期危急值以水、电解质和酸碱平衡紊乱最为常见,占43.2%(118/273),其中高钾血症最常见,占24.9%(68/273);出现危急值的男性比例高于女性(76.9%比23.1%),且多集中于35~54岁年龄段。对于出现高钾血症危急值患者,依次使用葡萄酸钙或氯化钙稳定心肌细胞膜、胰岛素、葡萄糖以及碳酸氢钠静脉滴注促使K+向细胞内转运、利尿药促进K+排泄,上述治疗无效则采用血液透析进行治疗。所有患者血钾均恢复正常。对出现其他危急值的患者,则针对不同情况采取个体化治疗措施。了解肾移植受者围手术期常见危急值,以及不同年龄段、不同性别的肾移植受者危急值分布的特点和原因,对临床监测和治疗有较强的指导作用。 Abstract:Objective To analyze and summarize the and charcteristics and processing methods of critical value in renal transplantation recipients during perioperative period. Methods Clinical data including gender, age, critical value, primary disease, clinical diagnosis and corresponding management at the presence of critical value in 273 cases with renal transplantation were collected and analyzed during perioperative period. Results and conclusions During perioperative period, the critical values of water, electrolyte and acid-base disorders were observed in 43.2% (118/273) of renal transplantation cases. The hyperpotassemia was found in 24.9% (68/273) of cases, which was the most common critical value. The percentage of male patients presenting with critical value was 76.9%, significantly higher compared with 23.1% in female counterparts, especially in those aged 35 to 54 years. For patients with critical value of hyperpotassemia, calcium gluconate or calcium chloride was administered to stabilize myocardium cell membrane. Insulin, glucose and sodium bicarbonate were administered via intravenous drip to accelerate intracellular transportation of K+ and diuretics were used to promote the excretion of K+. Hemodialysis therapy was used if the treatment is ineffective. The serum level of potassium restored to normal range after treatment in all cases. For those presenting with critical values of other parameters, individualized treatment was adopted based upon different conditions. Understanding of common critical values during perioperative period, characteristics and causes of distribution of critical values in renal transplant recipients of different age and gender offers guidance for clinical monitoring and treatment. -
Key words:
- Renal transplantation /
- Perioperative period /
- Critical value /
- Hyperpotassemia
-

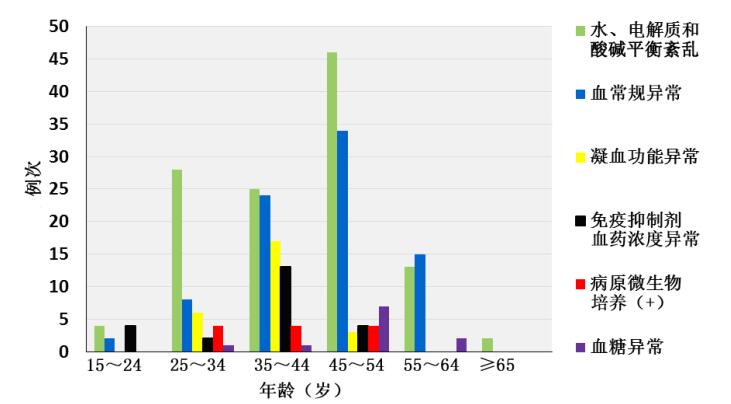
图 1 不同危急值项目年龄分布
Figure 1. Age distribution of patients with critical value in different items

图 2 肾移植受者围手术期不同危急值项目分布
Figure 2. Items distribution of perioperative renal transplant recipients with critical value

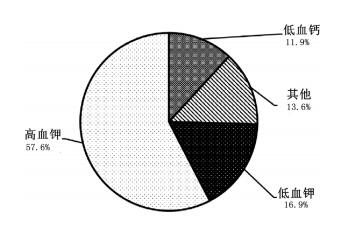
图 3 肾移植受者围手术期水、电解质失衡原因分布
Figure 3. Causes distribution of perioperative renal transplant recipients with metabolic disturbances and electrolyte abnormalities
表 1 肾移植受者围手术期不同危急值项目结果统计表
Table 1. Critical values of perioperative renal transplant recipients (n=273)
危急值项目 正常值参考范围 危急值范围 例次 频率(%) 水、电解质和酸碱平衡紊乱 K+ 3.50~5.30 mmol/L ≥6.5 mmol/L 68 24.9 ≤2.8 mmol/L 20 7.3 Ca2+ 2.20~2.65 mmol/L ≥3.50 mmol/L 2 0.7 ≤1.50 mmol/L 14 5.1 Na+ 137~147 mmol/L ≥160 mmol/L 2 0.7 ≤120 mmol/L 1 0.4 Cl- 99~110 mmol/L ≥125 mmol/L 1 0.4 TCO2 21~31 mmol/L ≥40 mmol/L 1 0.4 ≤10 mmol/L 8 2.9 pH 7.35~7.45 ≥7.55 1 0.4 免疫抑制剂血药浓度异常 FK506 0~20 ng/mL >20 ng/mL 21 7.7 MPA 0~15 ng/mL ≥15 ng/mL 2 0.7 血常规异常 Hb 130~175 g/L ≥180 g/L 9 3.3 ≤50 g/L 23 8.4 WBC 3.50~9.50×109 /L ≥30.00×109/L 20 7.3 ≤1.00×109/L 12 4.4 Plt 125~350×109/L <20×109/L 19 7.0 血糖异常 Glu 3.9~6.1 mmol/L ≥25.0 mmol/L 4 1.5 ≤2.2 mmol/L 7 2.6 凝血功能异常 PT 11~13 s >30 s 26 9.5 APTT 22.7~31.8 s >70.0 s 5* - FK506为他克莫司;MPA为霉酚酸;Hb为血红蛋白;WBC为白细胞;Plt为血小板;Glu为血糖;PT为凝血酶原时间;APTT为活化部分凝血活酶时间;*此数据包含在PT>30 s例次中  下载: 导出CSV
下载: 导出CSV
-
[1] Schapkaitz E, Levy B. Critical limits for urgent clinician notification at South African intensive care units[J]. Int J Lab Hematol, 2015, 37(5): 620-625. DOI: 10.1111/ijlh.12373. [2] 中国医院协会患者安全目标(2014-2015)[J].中国医院, 2014(10):22.Safety goals of patient in Chinese hospital association (2014-2015)[J]. Chin Hosp, 2014(10):22. [3] Kost GJ. Critical limits for emergency clinician notification at United States children's hospitals[J]. Pediatrics, 1991, 88(3):597-603. [4] Lien YH. Top 10 things primary care physicians should know about maintenance immunosuppression for transplant recipients[J]. Am J Med, 2016, 129(6):568-572. DIO 10.1016/j.amjmed.2015.11.034. doi: 10.1016/j.amjmed.2015.11.034 [5] Ayach T, Nappo RW, Paugh-Miller JL, et al. Postoperative hyperkalemia[J]. Eur J Intern Med, 2015, 26(2):106-111. DOI: 10.1016/j.ejim.2015.01.010 [6] Zanger R. Hyponatremia and hypokalemia in patients on peritoneal dialysis[J]. Semin Dial, 2010, 23(6):575-580. DOI: 10.11111/j.1525-139x.2010.00789.x. [7] Chatzopoulou A, Heijmans JP, Burgerhout E, et al. Glucocorticoid-induced attenuation of the inflammatory response in zebrafish[J]. Endocrinology, 2016: n2015-2050. DOI: 10.1210/en.2015-2050. [8] Srivastava A, Prabhakaran S, Sureka SK, et al. The challenges and outcomes of living donor kidney transplantation in pediatric and adolescent age group in a developing country: a critical analysis from a single center of north India[J]. Indian J Urol, 2015, 31(1):33-37. DOI: 10.4103/0970-1591.145290. [9] Baron D, Giral M, Brouard S. Reconsidering the detection of tolerance to individualize immunosuppression minimization and to improve long-term kidney graft outcomes[J]. Transpl Int, 2015, 28(8):938-959. DOI: 10.1111/tri.12578. [10] 谢云燕, 李亚林.危急值讨论制度在急诊留观病房中的应用[J].中华危重病急救医学, 2014, 26(5):357-359. DOI: 10.3760/cma.j.issn.2095-4352.2014.05.017.Xie YY, Li YL. Application of critical value discussion system in emergency wards under observation [J].Chin Crit Care Med, 2014, 26(5):357-359. DOI: 10.3760/cma.j.issn.2095-4352.2014.05.017. [11] 陈光意, 付书贞, 姜艳红, 等.河南省肿瘤医院血常规危急值统计分析[J].现代肿瘤医学, 2015(15): 2206-2208. DOI: 10.3969/j.issm. 1672-4992.2015.5.39.Chen GY, Chen FZ, Jiang YH, et al. The statistical analysis on critical value of blood routine examination in Henan Cancer Hospital[J]. J Mod Oncol, 2015(15):2206-2208. DOI: 10.3969/j.issm. 1672-4992.2015.5.39. [12] Kost GJ, Hale KN. Global trends in critical values practices and their harmonization[J]. Clin Chem Lab Med, 2011, 49(2):167-176. DOI: 10.1515/CCLM. 2011.033. [13] Agarwal R, Chhillar N, Tripathi CB. Study of variables affecting critical value notification in a laboratory catering to tertiary care hospital[J]. Indian J Clin Biochem, 2015, 30(1):89-93. DOI: 10.1007./S12291-013-0409-x. [14] Kopcinovic LM, Trifunovic J, Pavosevic T, et al. Croatian survey on critical results reporting[J]. Biochem Med, 2015, 25(2):193-202. DOI: 10.11613/BM.2015.019. [15] McFarlane A, Aslan B, Raby A, et al. Critical values in hematology[J]. Int J Lab Hematol, 2015, 37(1):36-43. DOI: 10.1111/ijlh.12226. [16] Zeng R, Wang W, Wang Z. National survey on critical values notification of 599 institutions in China[J]. Clin Chem Lab Med, 2013, 51(11):2099-2107. DOI: 10.1515/cclm-2013-0183. [17] Niu A, Yan X, Wang L, et al. Utility and necessity of repeat testing of critical values in the clinical chemistry laboratory[J]. PLoS One, 2013, 8(11):e80663. DOI: 10.1371/journal. pone.0080663. [18] 王丹, 王清涛, 郭健, 等.北京地区成人危急值界限值分布情况的调查研究[J].中华检验医学杂志, 2016, 39(3):181-186. DOI: 10.3760/cma.j.issn.1009-9158.2016.03.008.Wang D, Wang QT, Guo J, et al. Investigation on the distribution of critical value limits in adult patients in Beijing[J]. Chin J Lab Med, 2016, 39(3):181-186.DOI: 10.3760/cma.j.issn.1009-9158.2016.03.008. -

 下载:
下载:


 点击查看大图
点击查看大图
计量
- 文章访问数: 145
- HTML全文浏览量: 31
- PDF下载量: 9
- 被引次数: 0


