

Comprehensive minimally invasive treatment for biliary anastomotic stenosis after orthotopic liver transplantation: a single center analysis of 60 cases
-
摘要:
目的 探讨以内镜逆行胆胰管造影术(ERCP)为主的综合微创方案治疗肝移植术后胆道吻合口狭窄(BAS)的临床效果。 方法 回顾性分析60例肝移植术后BAS受者的资料,其中男54例,女6例,年龄(48±10)岁。首先采用ERCP治疗,成功后放置胆道塑料或金属支架,失败者选择经皮经肝胆道引流术(PTCD)会师法或经口单人操作胆道镜(SpyGlass)通过狭窄,以上均失败者则进行磁吻合再通法或其他特殊方法。总结肝移植术后BAS的发生及治疗情况,分析治疗结果、脱支架情况及复发情况。 结果 肝移植术后发生BAS的中位时间为8(4,13)个月,术后1年内、1~2年及2年以上诊断BAS的受者分别为39例、16例及5例。60例肝移植术后BAS受者均得到成功救治,其中56例首先进行ERCP,41例完成BAS治疗,成功率为73%,导丝不能通过是ERCP失败的主要原因;PTCD、SpyGlass及磁吻合再通法的成功率分别为5/9、5/7及7/8;2例通过经皮胆道镜导丝钝头突破技术和胆道十二指肠内瘘口放置支架治疗成功。38例经过3(3,4)次ERCP、13(8,18)个月支架留置后达到脱支架标准,其中塑料支架25例,金属支架13例,塑料支架留置时间较金属支架长(P < 0.05)。6例在脱支架后12(8,33)个月狭窄复发,复发率为16%。复发者再次ERCP治疗,5例成功脱支架无复发。多因素分析结果提示狭窄诊断时间迟、脱支架前ERCP治疗次数多是BAS复发的独立危险因素(均为P < 0.05)。 结论 以ERCP为主的综合微创方案可提高肝移植术后BAS治疗成功率,远期效果满意,BAS诊断时间迟、脱支架所需ERCP次数多是BAS复发的独立危险因素。 -
关键词:
- 肝移植 /
- 胆道吻合口狭窄 /
- 微创治疗 /
- 内镜逆行胆胰管造影术(ERCP) /
- 经皮经肝胆道引流术(PTCD) /
- 经口单人操作胆道镜(SpyGlass) /
- 磁吻合 /
- 经皮经肝胆道镜 /
- 金属支架 /
- 塑料支架
Abstract:Objective To evaluate the clinical efficacy of endoscopic retrograde cholangiopancreatography (ERCP)-based comprehensive minimally invasive treatment for biliary anastomotic stenosis (BAS) after liver transplantation. Methods Clinical data of 60 BAS recipients after liver transplantation were retrospectively analyzed, 54 male and 6 female, aged (48±10) years. ERCP was initially carried out. If it succeeded, plastic or metallic stents were placed into the biliary tract. If it failed, percutaneous transhepatic cholangial drainage (PTCD) or single-operator cholangioscopy (SpyGlass) was adopted to pass through the stenosis. If all these procedures failed, magnetic anastomosis or other special methods were delivered. The incidence and treatment of BAS after liver transplantation were summarized. The efficacy, stent removal and recurrence were observed. Results The median time of incidence of BAS after liver transplantation was 8 (4, 13) months. Within postoperative 1 year, 1-2 years and over 2 years, 39, 16 and 5 recipients were diagnosed with BAS, respectively. All 60 BAS recipients after liver transplantation were successfully treated, including 56 cases initially receiving ERCP, and 41 completing BAS treatment, with a success rate of 73%. The failure of guide wire was the main cause of ERCP failure. The success rates of PTCD, SpyGlass and magnetic anastomosis were 5/9, 5/7 and 7/8, respectively. Two recipients were successfully treated by percutaneous choledochoscope-assisted blunt guide wire technique and stent placement in the biliary and duodenal fistula. After 3 (3, 4) cycles of ERCP and 13 (8, 18) months of stent indwelling, 38 recipients reached the stent removal criteria, including 25 plastic stents and 13 metallic stents. The indwelling time of plastic stents was longer than that of metallic stents (P < 0.05). Six cases suffered from stenosis recurrence at 12 (8, 33) months after stent removal, and the recurrence rate was 16%. Six patients were treated with ERCP, and 5 of them did not recur after the stents were successfully removed. Multivariate analysis showed that delayed diagnosis of stenosis and frequent ERCP before stent removal were the independent risk factors for BAS recurrence (both P < 0.05). Conclusions ERCP-based comprehensive minimally invasive treatment may improve the success rate of BAS treatment after liver transplantation and yield satisfactory long-term efficacy. Delayed diagnosis of BAS and high frequent ERCP required for stent removal are the independent risk factors for BAS recurrence. -
Key words:
- Liver Transplantation /
- Biliary anastomotic stricture /
- Minimally invasive treatment /
- Endoscopic retrograde cholangiopancreatography(ERCP) /
- Percutaneous transhepatic cholangial drainage(PTCD) /
- Single-operator cholangioscopy (SpyGlass) /
- Magnetic anastomosis /
- Percutaneous transhepatic cholangioscopy /
- Metallic stent /
- Plastic stent
-

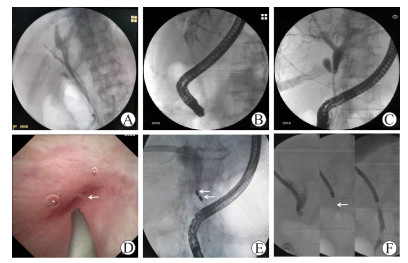
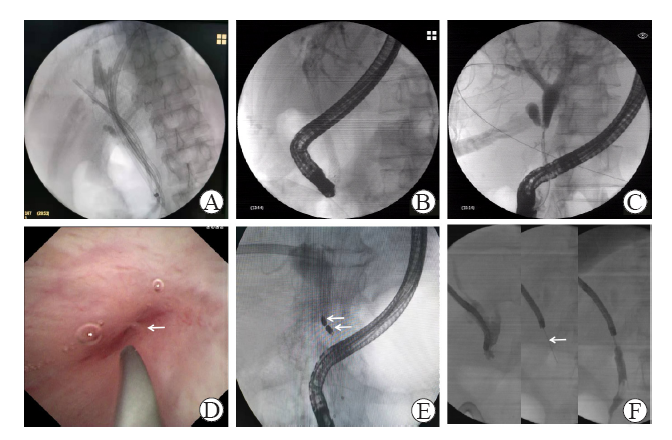
图 1 肝移植术后BAS的治疗方法
注:A图为ERCP+多支塑料支架;B图为ERCP+胆道全覆膜金属支架;C图为PTCD会师技术;D图为SpyGlass辅助导丝超选重度狭窄(箭头示中心性针尖样狭窄);E图为磁吻合再通(箭头示子母磁体);F图为经皮经肝胆道镜引导导丝钝头突破技术(箭头示导丝钝头)。
Figure 1. Treatment of BAS after liver transplantation

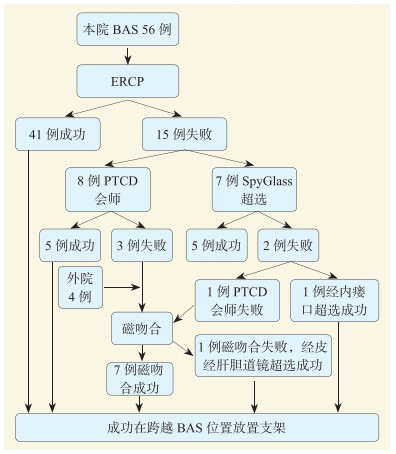
图 2 本组肝移植术后BAS受者治疗流程
Figure 2. Treatment process of BAS recipients after liver transplantation in this group
表 1 脱支架后BAS复发危险因素的单因素分析
Table 1. Univariate analysis of risk factors for recurrence of BAS after stent removal
临床因素 例数 复发例数 Wald值 比值比 95%可信区间 P值 性别 6.382 0.238 0.078~0.725 0.012 男 34 5 女 4 1 年龄① - - 1.542 0.971 0.926~1.017 0.214 支架类型 3.112 2.258 0.913~5.582 0.078 塑料支架 25 3 金属支架 13 3 磁吻合 0.394 1.483 0.433~5.081 0.530 是 6 1 否 32 5 T管引流 0.774 1.569 0.575~4.276 0.379 是 8 1 否 30 5 胆瘘 1.240 1.777 0.646~4.888 0.265 是 7 1 否 31 5 ERCP治疗次数① - - 21.061 2.752 1.786~4.241 < 0.001 支架留置时间① - - 0.149 1.017 0.934~1.108 0.700 狭窄诊断时间① - - 4.588 1.028 1.002~1.054 0.032 注:①为连续变量。  下载: 导出CSV
下载: 导出CSV
表 2 脱支架后BAS复发危险因素的多因素分析
Table 2. Multivariate analysis of risk factors for recurrence of BAS after stent removal
临床因素 B值 标准误 Wald值 比值比 95%可信区间 P值 狭窄诊断时间 0.044 0.017 6.823 1.045 1.011~1.080 0.009 ERCP治疗次数 1.250 0.258 23.389 3.490 2.103~5.792 < 0.001 常量 -7.080 1.201 34.756 0.001 -① < 0.001 注:①-为无数据。
下载: 导出CSV
-
[1] FORDE JJ, BHAMIDIMARRI KR. Management of biliary complications in liver transplant recipients[J]. Clin Liver Dis, 2022, 26(1): 81-99. DOI: 10.1016/j.cld.2021.08.008. [2] GUIRGUIS RN, NASHAAT EH, YASSIN AE, et al. Biliary complications in recipients of living donor liver transplantation: a single-centre study[J]. World J Hepatol, 2021, 13(12): 2081-2103. DOI: 10.4254/wjh.v13.i12.2081. [3] VERDONK RC, BUIS CI, PORTE RJ, et al. Anastomotic biliary strictures after liver transplantation: causes and consequences[J]. Liver Transpl, 2006, 12(5): 726-735. DOI: 10.1002/lt.20714. [4] BOEVA I, KARAGYOZOV PI, TISHKOV I. Post-liver transplant biliary complications: current knowledge and therapeutic advances[J]. World J Hepatol, 2021, 13(1): 66-79. DOI: 10.4254/wjh.v13.i1.66. [5] PARLAK E, SIMSEK C, KOKSAL AS, et al. The classification of biliary strictures in patients with right-lobe liver transplant recipients and its relation to traversing the stricture with a guidewire[J]. Transplantation, 2022, 106(2): 328-336. DOI: 10.1097/TP.0000000000003738. [6] KIMURA K, YOSHIZUMI T, KUDO K, et al. Intractable biliary strictures after living donor liver transplantation: a case series[J]. Transplant Proc, 2021, 53(5): 1726-1730. DOI: 10.1016/j.transproceed.2021.04.015. [7] KOKSAL AS, EMINLER AT, PARLAK E, et al. Management of biliary anastomotic strictures after liver transplantation[J]. Transplant Rev (Orlando), 2017, 31(3): 207-217. DOI: 10.1016/j.trre.2017.03.002. [8] 郝杰, 李宇, 陶杰, 等. 胆道支架在内镜逆行胰胆管造影治疗肝移植术后胆道良性狭窄中的应用价值[J]. 中华消化外科杂志, 2017, 16(4): 385-390. DOI: 10.3760/cma.j.issn.1673-9752.2017.04.014.HAO J, LI Y, TAO J, et al. Application value of biliary stent in endoscopic retrograde cholangio pancreatography for treatment of benign biliary stricture after liver transplantation[J]. Chin J Dig Surg, 2017, 16(4): 385-390. DOI: 10.3760/cma.j.issn.1673-9752.2017.04.014. [9] LI Y, SUN H, YAN X, et al. Magnetic compression anastomosis for the treatment of benign biliary strictures: a clinical study from China[J]. Surg Endosc, 2020, 34(6): 2541-2550. DOI: 10.1007/s00464-019-07063-8. [10] 李宇, 孙昊, 严小鹏, 等. 磁压榨吻合治疗六例良性胆管狭窄[J]. 中华消化杂志, 2018, 38(12): 848-851. DOI: 10.3760/cma.j.issn.0254-1432.2018.12.012.LI Y, SUN H, YAN XP, et al. Treatment of benign bile duct stricture by magnetic press anastomosis in 6 cases[J]. Chin J Dig, 2018, 38(12): 848-851. DOI: 10.3760/cma.j.issn.0254-1432.2018.12.012. [11] 中华医学会消化内镜学分会ERCP学组, 中国医师协会消化医师分会胆胰学组, 国家消化系统疾病临床医学研究中心. 中国ERCP指南(2018版)[J]. 中华消化内镜杂志, 2018, 35(11): 777-813. DOI: 10.3760/cma.j.issn.1007-5232.2018.11.001.ERCP Group of Digestive Endoscopy Society of Chinese Medical Association, Biliopancreatic Group of Gastroenterologist Society of Chinese Medical Doctor Association, National Clinical Medical Research Center of Digestive System Diseases. ERCP guideline of China (2018 edition)[J]. Chin J Dig Endosc, 2018, 35(11): 777-813. DOI: 10.3760/cma.j.issn.1007-5232.2018.11.001. [12] JARLOT-GAS C, MUSCARI F, MOKRANE FZ, et al. Management of anastomotic biliary stricture after liver transplantation and impact on survival[J]. HPB (Oxford), 2021, 23(8): 1259-1268. DOI: 10.1016/j.hpb.2020.12.008. [13] KARATOPRAK S, KUTLU R, KARATOPRAK NB, et al. Percutaneous radiological biliary interventions after failed endoscopic treatment in living liver donors: experience of a high-volume transplantation center[J]. Transpl Int, 2021, 34(12): 2846-2855. DOI: 10.1111/tri.14118. [14] KARATOPRAK S, KUTLU R, YILMAZ S. Role of percutaneous radiological treatment in biliary complications associated with adult left lobe living donor liver transplantation: a single-center experience[J]. Diagn Interv Radiol, 2021, 27(4): 546-552. DOI: 10.5152/dir.2021.20523. [15] LEE SH, RYU JK, WOO SM, et al. Optimal interventional treatment and long-term outcomes for biliary stricture after liver transplantation[J]. Clin Transplant, 2008, 22(4): 484-493. DOI: 10.1111/j.1399-0012.2008.00813.x. [16] MARTINS FP, SELETI SMR, CONTINI ML, et al. Is there a place for cholangioscopic evaluation of biliary anastomotic stricture after deceased donor liver transplant?[J]. Arq Gastroenterol, 2020, 57(4): 347-353. DOI: 10.1590/S0004-2803.202000000-67. [17] 赵东, 张卓, 黄一鸣, 等. SpyGlass直视系统在肝移植术后胆道狭窄诊治中的初步探索[J]. 器官移植, 2022, 13(1): 55-60. DOI: 10.3969/j.issn.1674-7445.2022.01.009.ZHAO D, ZHANG Z, HUANG YM, et al. Preliminary exploration of SpyGlass direct visualization system in diagnosis and treatment of biliary stricture after liver transplantation[J]. Organ Transplant, 2022, 13(1): 55-60. DOI: 10.3969/j.issn.1674-7445.2022.01.009. [18] BOKEMEYER A, GROSS D, BRÜCKNER M, et al. Digital single-operator cholangioscopy: a useful tool for selective guidewire placements across complex biliary strictures[J]. Surg Endosc, 2019, 33(3): 731-737. DOI: 10.1007/s00464-018-6334-6. [19] 李宇, 董鼎辉, 刘学民, 等. 胆道镜下导丝突破法治疗困难胆管吻合口狭窄12例疗效分析[J]. 中国实用外科杂志, 2022, 42(4): 404-408. DOI: 10.19538/j.cjps.issn1005-2208.2022.04.08.LI Y, DONG DH, LIU XM, et al. Treatment of difficult bile duct anastomotic stricture with guide wire breakthrough under choledochoscope: an analysis of 12 cases[J]. Chin J Pract Surg, 2022, 42(4): 404-408. DOI: 10.19538/j.cjps.issn1005-2208.2022.04.08. [20] 中华医学会外科学分会外科手术学学组. 关于利用磁力再通术治疗肝移植术后胆道吻合口狭窄的专家建议[J]. 器官移植, 2020, 11(1): 13-18. DOI: 10.3969/j.issn.1674-7445.2020.01.003.Operative Surgery Group of Branch of Surgery of Chinese Medical Association. Expert recommendation on magnetic recanalization for the treatment of biliary anastomosis stricture after liver transplantation[J]. Organ Transplant, 2020, 11(1): 13-18. DOI: 10.3969/j.issn.1674-7445.2020.01.003. [21] JANG SI, CHO JH, LEE DK. Magnetic compression anastomosis for the treatment of post-transplant biliary stricture[J]. Clin Endosc, 2020, 53(3): 266-275. DOI: 10.5946/ce.2020.095. [22] 时之梅, 陈萃, 吴军, 等. 磁性压迫融合术在肝移植术后胆道吻合口狭窄中的应用一例[J]. 中华消化内镜杂志, 2020, 37(12): 942-943. DOI: 10.3760/cma.j.cn321463-20191008-00671.SHI ZM, CHEN C, WU J, et al. Application of magnetic compression fusion in biliary anastomotic stricture after liver transplantation: a case report[J]. Chin J Dig Endosc, 2020, 37(12): 942-943. DOI: 10.3760/cma.j.cn321463-20191008-00671. [23] MARTINS FP, DE PAULO GA, CONTINI MLC, et al. Metal versus plastic stents for anastomotic biliary strictures after liver transplantation: a randomized controlled trial[J]. Gastrointest Endosc, 2018, 87(1): 131. e1-131. e13. DOI: 10.1016/j.gie.2017.04.013. [24] TAL AO, FINKELMEIER F, FILMANN N, et al. Multiple plastic stents versus covered metal stent for treatment of anastomotic biliary strictures after liver transplantation: a prospective, randomized, multicenter trial[J]. Gastrointest Endosc, 2017, 86(6): 1038-1045. DOI: 10.1016/j.gie.2017.03.009. [25] CANTÙ P, SANTI G, ROSA R, et al. Cost analysis of a long-term randomized controlled study in biliary duct-to-duct anastomotic stricture after liver transplantation[J]. Transpl Int, 2021, 34(5): 825-834. DOI: 10.1111/tri.13867. [26] VISCONTI TAC, BERNARDO WM, MOURA DTH, et al. Metallic vs plastic stents to treat biliary stricture after liver transplantation: a systematic review and Meta-analysis based on randomized trials[J]. Endosc Int Open, 2018, 6(8): E914-E923. DOI: 10.1055/a-0626-7048. [27] KAMAL F, ALI KHAN M, LEE-SMITH W, et al. Metal versus plastic stents in the management of benign biliary strictures: systematic review and Meta-analysis of randomized controlled trials[J]. Eur J Gastroenterol Hepatol, 2022, 34(5): 478-487. DOI: 10.1097/MEG.0000000000002352. [28] KAO D, ZEPEDA-GOMEZ S, TANDON P, et al. Managing the post-liver transplantation anastomotic biliary stricture: multiple plastic versus metal stents: a systematic review[J]. Gastrointest Endosc, 2013, 77(5): 679-691. DOI: 10.1016/j.gie.2013.01.015. [29] KOHLI DR, HARRISON ME, MUJAHED T, et al. Outcomes of endoscopic therapy in donation after cardiac death liver transplant biliary strictures[J]. HPB (Oxford), 2020, 22(7): 979-986. DOI: 10.1016/j.hpb.2019.10.018. [30] ALAZMI WM, FOGEL EL, WATKINS JL, et al. Recurrence rate of anastomotic biliary strictures in patients who have had previous successful endoscopic therapy for anastomotic narrowing after orthotopic liver transplantation[J]. Endoscopy, 2006, 38(6): 571-574. DOI: 10.1055/s-2006-925027. [31] SATAPATHY SK, SHEIKH I, ALI B, et al. Long-term outcomes of early compared to late onset choledochocholedochal anastomotic strictures after orthotopic liver transplantation[J]. Clin Transplant, 2017, 31(7): e13003. DOI: 10.1111/ctr.13003. -

 下载:
下载:

 点击查看大图
点击查看大图
计量
- 文章访问数: 234
- HTML全文浏览量: 163
- PDF下载量: 81
- 被引次数: 0


