

Establishment and effect evaluation of risk prediction model for lung infection after kidney transplantation
-
摘要:
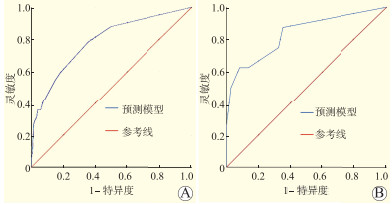
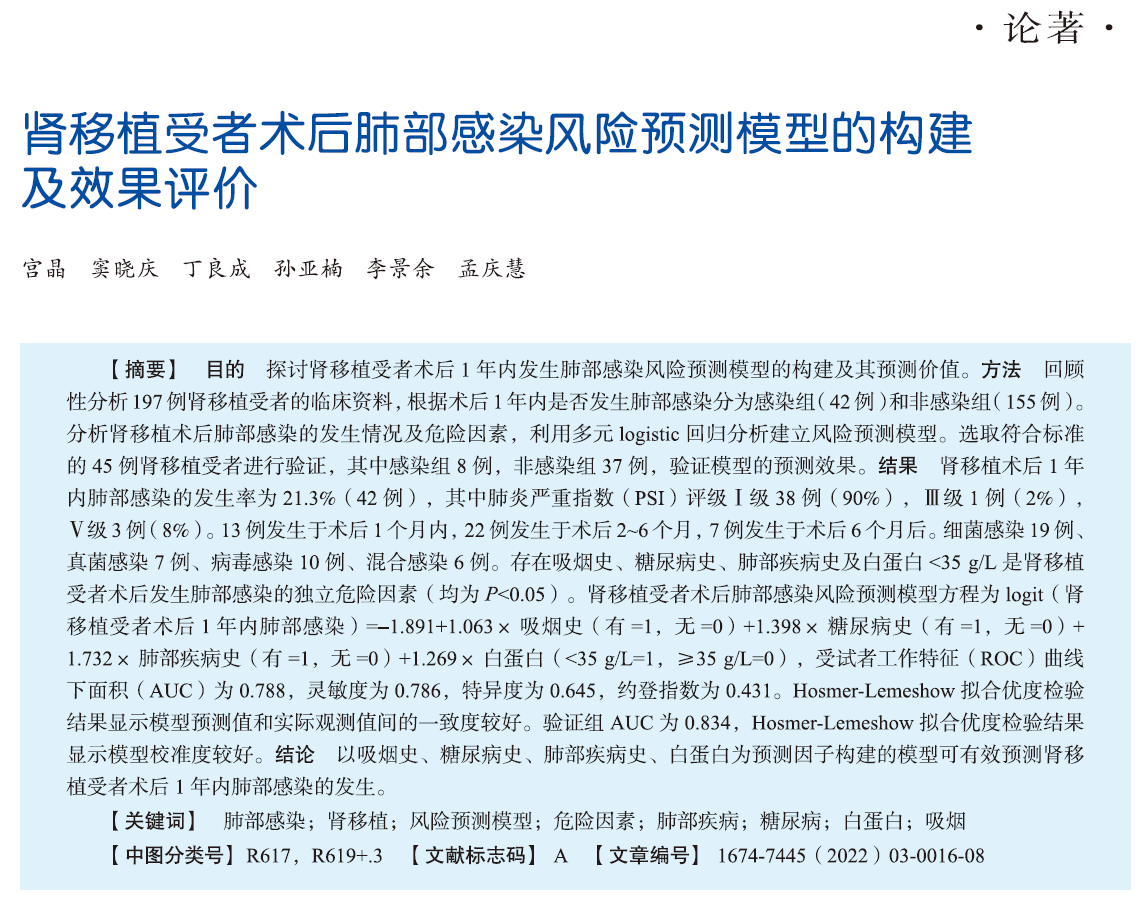
目的 探讨肾移植受者术后1年内发生肺部感染风险预测模型的构建及其预测价值。 方法 回顾性分析197例肾移植受者的临床资料,根据术后1年内是否发生肺部感染分为感染组(42例)和非感染组(155例)。分析肾移植术后肺部感染的发生情况及危险因素,利用多元logistic回归分析建立风险预测模型。选取符合标准的45例肾移植受者进行验证,其中感染组8例,非感染组37例,验证模型的预测效果。 结果 肾移植术后1年内肺部感染的发生率为21.3%(42例),其中肺炎严重指数(PSI)评级Ⅰ级38例(90%),Ⅲ级1例(2%),Ⅴ级3例(8%)。13例发生于术后1个月内,22例发生于术后2~6个月,7例发生于术后6个月后。细菌感染19例、真菌感染7例、病毒感染10例、混合感染6例。存在吸烟史、糖尿病史、肺部疾病史及白蛋白 < 35 g/L是肾移植受者术后发生肺部感染的独立危险因素(均为P < 0.05)。肾移植受者术后肺部感染风险预测模型方程为logit(肾移植受者术后1年内肺部感染)=-1.891+1.063×吸烟史(有=1,无=0)+1.398×糖尿病史(有=1,无=0)+1.732×肺部疾病史(有=1,无=0)+1.269×白蛋白(< 35 g/L=1,≥35 g/L=0),受试者工作特征(ROC)曲线下面积(AUC)为0.788,灵敏度为0.786,特异度为0.645,约登指数为0.431。Hosmer-Lemeshow拟合优度检验结果显示模型预测值和实际观测值间的一致度较好。验证组AUC为0.834,Hosmer-Lemeshow拟合优度检验结果显示模型校准度较好。 结论 以吸烟史、糖尿病史、肺部疾病史、白蛋白为预测因子构建的模型可有效预测肾移植受者术后1年内肺部感染的发生。 Abstract:Objective To establish and evaluate the predictive value of the risk prediction model for lung infection within postoperative 1 year in kidney transplant recipients. Methods Clinical data of 197 kidney transplant recipients were retrospectively analyzed. All recipients were divided into the infection group (n=42) and non-infection group (n=155) according to the incidence of lung infection within postoperative 1 year. The incidence and risk factors of lung infection after kidney transplantation were analyzed. Risk prediction model was established by multiple logistic regression analysis. Forty-five kidney transplant recipients who met the inclusion criteria, including 8 cases in the infection group and 37 cases in the non-infection group, were selected to verify the predictive effect of the established model. Results The incidence of lung infection within 1 year after kidney transplantation was 21.3% (n=42), including 38 cases (90%) of pneumonia severity index (PSI) class Ⅰ, 1 case (2%) of PSI class Ⅲ and 3 cases (8%) of PSI class Ⅴ. Lung infection occurred within 1 month after operation in 13 cases, within postoperative 2-6 months in 22 cases and after postoperative 6 months in 7 cases. Nineteen recipients were diagnosed with bacterial infection, 7 cases of fungal infection, 10 cases of viral infection and 6 cases of mixed infection. Smoking history, diabetes mellitus history, pulmonary disease history and albumin level of < 35 g/L were the independent risk factors for lung infection after kidney transplantation (all P < 0.05). The equation of risk prediction model for postoperative lung infection in kidney transplant recipients was logit (lung infection within postoperative 1 year in kidney transplant recipients)=-1.891+1.063×smoking history (yes=1, no=0)+1.398×diabetes mellitus history (yes=1, no=0)+1.732×pulmonary disease history (yes=1, no=0)+1.269×albumin level (< 35 g/L=1, ≥35 g/L=0). The area under the curve (AUC) of receiver operating characteristic (ROC) was 0.788, the sensitivity was 0.786, the specificity was 0.645, and the Youden index was 0.431, respectively. Hosmer-Lemeshow goodness-of-fit test demonstrated that the predicted value of this model yielded relatively high consistency with the observed value. The AUC in the verification group was 0.834. Hosmer-Lemeshow goodness-of-fit test validated high degree of calibration of this model. Conclusions The risk prediction model, consisting of smoking history, diabetes mellitus history, pulmonary disease history and albumin level as predictors, may effectively predict the incidence of lung infection within postoperative 1 year in kidney transplant recipients. -
Key words:
- Lung infection /
- Kidney transplantation /
- Risk prediction model /
- Risk factor /
- Pulmonary disease /
- Diabetes mellitus /
- Albumin /
- Smoking
-

图 1 模型组和验证组肾移植受者术后发生肺部感染的ROC曲线
注:A图为模型组ROC曲线;B图为验证组ROC曲线。
Figure 1. ROC curves of postoperative pulmonary infection in kidney transplant recipients in model group and validation group
表 1 肾移植术后发生肺部感染危险因素的单因素分析
Table 1. Univariate analysis of risk factors for pulmonary infection after kidney transplantation
变量 感染组(n=42) 非感染组(n=155) 统计值 P值 变量 感染组(n=42) 非感染组(n=155) 统计值 P值 年龄[M(P25,P75),岁] 43(34,51) 42(34,48) 0.232 0.871 术前透析[n(%)] 0.000 1.000 性别[n(%)] 0.287 0.592 有 41(98) 151(97) 男 30(71) 117(75) 无 1(2) 4(3) 女 12(29) 38(25) 术前诱导方案[n(%)] 0.436 0.509 BMI[n(%)] 0.660 0.509 巴利昔单抗 8(19) 37(24) < 18 kg/m2 13(31) 54(35) 抗人T淋巴细胞球蛋白 34(81) 118(76) 18~24 kg/m2 24(57) 88(57) 围手术期误吸[n(%)] 7.987 0.005 > 24 kg/m2 5(12) 13(8) 有 5(12) 2(1) 吸烟史[n(%)] 14.272 < 0.001 无 37(88) 153(99) 有 22(52) 35(23) 术前使用抗菌药物[n(%)] 0.000 1.000 无 20(48) 120(77) 有 42(100) 154(99) 酗酒史[n(%)] 2.139 0.343 无 0 1(1) 有 2(5) 19(12) 白细胞[n(%)] 1.048 0.295 无 40(95) 136(88) < 4×109/L 1(2) 3(2) 原发疾病病程[n(%)] 1.183 0.237 4~10×109/L 21(50) 64(41) < 1年 3(7) 27(17) > 10×109/L 20(48) 88(57) 2~5年 21(50) 70(45) 淋巴细胞绝对值[n(%)] 0.714 0.475 > 5年 18(43) 58(37) < 0.8×109/L 39(93) 148(95) 供者来源[n(%)] 0.436 0.509 0.8~3.5×109/L 2(5) 7(5) 亲属活体 8(19) 37(24) > 3.5×109/L 1(2) 0 脑死亡供者 34(81) 118(76) 白蛋白[n(%)] 13.391 < 0.001 高血压史[n(%)] 4.265 0.039 < 35 g/L 24(57) 42(27) 有 33(79) 140(90) ≥35 g/L 18(43) 113(73) 无 9(21) 15(10) 血清肌酐[n(%)] 1.527 0.217 糖尿病史[n(%)] 18.891 < 0.001 ≤110 μmoI/L 3(7) 3(2) 有 14(33) 12(8) > 110 μmoI/L 39(93) 152(98) 无 28(67) 143(92) 供肾脓液培养病原菌[n(%)] 0.614 0.433 肺部疾病史[n(%)] 10.311 0.001 有 21(50) 67(43) 有 10(24) 9(6) 无 21(50) 88(57) 无 32(76) 146(94) 注:白细胞、淋巴细胞绝对值、白蛋白、血清肌酐均为肾移植术后第1次测量结果。  下载: 导出CSV
下载: 导出CSV
表 2 肾移植术后发生肺部感染危险因素的多因素分析
Table 2. Multivariate analysis of risk factors for pulmonary infection after kidney transplantation
危险因素 偏回归系数 标准误 Wald χ2 P值 OR①值 95%CI② 常数项 -1.891 0.585 10.459 0.001 0.151 -③ 吸烟史 1.063 0.423 6.329 0.012 2.896 1.265~6.633 高血压史 -1.050 0.596 3.109 0.078 0.350 0.109~1.124 糖尿病史 1.398 0.522 7.183 0.007 4.407 1.456~11.250 肺部疾病史 1.732 0.567 9.342 0.002 6.121 1.861~17.156 围手术期误吸 2.061 1.122 3.372 0.066 7.851 0.871~70.813 白蛋白 < 35 g/L 1.269 0.425 8.917 0.003 3.566 1.546~8.178 注:①OR为比值比。
②CI为可信区间。
③-为无数据。
下载: 导出CSV
表 3 模型组和验证组危险因素比较
Table 3. Comparison of risk factors between model group and validation group
变量 模型组(n=197) 验证组(n=45) 统计值 P值 吸烟史[n(%)] 0.245 0.283 有 57(29) 17(38) 无 140(71) 28(62) 糖尿病史[n(%)] 0.626 0.616 有 26(13) 4(9) 无 171(87) 41(91) 肺部疾病史[n(%)] 0.596 0.687 有 42(21) 8(18) 无 155(79) 37(82) 白蛋白[n(%)] 0.586 0.604 < 35 g/L 66(34) 17(38) ≥35 g/L 131(66) 28(62)
下载: 导出CSV
-
[1] KINNUNEN S, KARHAPÄÄ P, JUUTILAINEN A, et al. Secular trends in infection-related mortality after kidney transplantation[J]. Clin J Am Soc Nephrol, 2018, 13(5)755-762. DOI: 10.2215CJN.11511017. [2] SHIH CJ, TARNG DC, YANG WC, et al. Immunosuppressant dose reduction and long-term rejection risk in renal transplant recipients with severe bacterial pneumonia[J]. Singapore Med J, 2014, 55(7): 372-377. DOI: 10.11622/smedj.2014089. [3] 于立新, 曾明星. 肾移植术后肺部真菌感染的临床分析[J]. 南方医科大学学报, 2016, 36(6): 880-883. DOI: 10.3969/j.issn.1673-4254.2016.06.26.YU LX, ZENG MX. Pulmonary fungal infection after renal transplantation: analysis of 40 cases[J]. J Southern Med Univ, 2016, 36(6): 880-883. DOI: 10.3969/j.issn.1673-4254.2016.06.26. [4] 王鑫, 崔向丽, 杨辉, 等. 肾移植术后肺部感染的研究现状[J]. 中国临床药理学杂志, 2017, 33(3): 276-279. DOI: 10.13699/j.cnki.1001-6821.2017.03.024.WANG X, CUI XL, YANG H, et al. Research status of pulmonary infection after renal transplantation[J]. Chin J Clin Pharmacol, 2017, 33(3): 276-279. DOI: 10.13699/j.cnki.1001-6821.2017.03.024. [5] 邓聪, 孙卫民, 林梅双, 等. 肾移植术后肺部感染患者病原体及危险因素分析[J]. 河北医学, 2021, 27(2): 279-283. DOI: 10.3969/j.issn.1006-6233.2021.02.022.DENG C, SUN WM, LIN MS, et al. An analysis of pathogen spectrum and risk factors for pulmonary infection in kidney transplant recipients[J]. Hebei Med, 2021, 27(2): 279-283. DOI: 10.3969/j.issn.1006-6233.2021.02.022. [6] 潘佳善, 苏涌, 朱道方, 等. 公民逝世捐献与活体捐献肾移植的近期临床效果[J]. 实用医学杂志, 2022, 38(2): 184-189. DOI: 10.3969/j.issn.1006-5725.2022.02.011.PAN JS, SU Y, ZHU DF, et al. Clinical effects of deceased vs living donor on kidney transplantation[J]. J Pract Med, 2022, 38(2): 184-189. DOI: 10.3969/j.issn.1006-5725.2022.02.011. [7] 中华人民共和国卫生部. 医院感染诊断标准(试行)[J]. 中华医学杂志, 2001, 81(5): 314-320. https://www.cnki.com.cn/Article/CJFDTOTAL-ZHYX200105025.htmMinistry of Health of the People's Republic of China. Diagnostic criteria for nosocomial infections (proposed)[J]. Nat Med J China, 2001, 81(5): 314-320. https://www.cnki.com.cn/Article/CJFDTOTAL-ZHYX200105025.htm [8] 李智斌, 张更, 马帅军, 等. 3种肺部感染评分系统在肾移植术后肺部感染中的应用价值比较[J]. 器官移植, 2016, 7(3): 196-200. DOI: 10.3969/j.issn.1674-7445.2016.03.007.LI ZB, ZHANG G, MA SJ, et al. Comparison of application value of three pulmonary infection scoring systems in pulmonary infection after renal transplantation[J]. Organ Transplant, 2016, 7(3): 196-200. DOI: 10.3969/j.issn.1674-7445.2016.03.007. [9] MARTINS BCC, MESQUITA KHC, COSTA IHFD, et al. Hospital cost of complications after kidney transplant[J]. Transplant Proc, 2020, 52(5): 1294-1298. DOI: 10.1016/j.transproceed.2020.02.070. [10] 胡风侠. 肾移植后受者感染危险因素调查及直接经济负担研究[D]. 西安: 空军军医大学, 2018. [11] 段智梅, 姜淑娟, 邵杨, 等. 肾移植患者术后肺部感染的临床特征分析[J]. 中华医院感染学杂志, 2018, 28(20): 3107-3110. DOI: 10.11816/cn.ni.2018-173553.DUAN ZM, JIANG SJ, SHAO Y, et al. Clinical characteristics of patients with pulmonary infection after renal transplantation[J]. Chin J Nosocomiol, 2018, 28(20): 3107-3110. DOI: 10.11816/cn.ni.2018-173553. [12] 贺雪梅, 储爱琴, 王玉, 等. 肾移植受者术后感染的回顾性研究[J]. 中国临床保健杂志, 2021, 24(1): 121-124. DOI: 10.3969/J.issn.1672-6790.2021.01.031.HE XM, CHU AQ, WANG Y, et al. Retrospective study of secondary infections among kidney transplant recipients[J]. Chin J Clin Healthcare, 2021, 24(1): 121-124. DOI: 10.3969/J.issn.1672-6790.2021.01.031. [13] 刘佳, 李建军, 龙建华, 等. 肾移植术后肺部感染的临床特征及对肾功能的影响分析[J]. 中国现代医生, 2020, 58(32): 24-27. https://www.cnki.com.cn/Article/CJFDTOTAL-ZDYS202032008.htmLIU J, LI JJ, LONG JH, et al. Analysis on the clinical features of pulmonary infection after renal transplantation and its impacts on renal function[J]. China Mod Doc, 2020, 58(32): 24-27. https://www.cnki.com.cn/Article/CJFDTOTAL-ZDYS202032008.htm [14] MANGALGI S, MADAN K, DAS CJ, et al. Pulmonary infections after renal transplantation: a prospective study from a tropical country[J]. Transpl Int, 2021, 34(3): 525-534. DOI: 10.1111/tri.13817. [15] 兰天池. 单中心肾移植围手术期肺部感染的诊疗分析[D]. 合肥: 安徽医科大学, 2021. [16] 潘灵爱, 张晓勤. 肾移植术后肺部感染的高危因素分析[J]. 中国医刊, 2018, 53(12): 1346-1348. DOI: 10.3969/j.issn.1008-1070.2018.12.012.PAN LA, ZHANG XQ. Analysis on risk factors of pulmonary infection after renal transplantation[J]. Chin J Med, 2018, 53(12): 1346-1348. DOI: 10.3969/j.issn.1008-1070.2018.12.012. [17] PÉREZ-JACOISTE ASÍN MA, LÓPEZ-MEDRANO F, FERNÁNDEZ-RUIZ M, et al. Risk factors for the development of invasive aspergillosis after kidney transplantation: systematic review and Meta-analysis[J]. Am J Transplant, 2021, 21(2): 703-716. DOI: 10.1111/ajt.16248. [18] 刘彦妤, 岳慧杰, 陈晨, 等. 肾移植受者围手术期感染危险因素及预防用抗菌药物合理性的分析[J]. 医学研究生学报, 2020, 33(11): 1181-1186. DOI: 10.16571/j.cnki.1008-8199.2020.11.012.LIU YY, YUE HJ, CHEN C, et al. Analysis of perioperative infection risk factors and rationality of prophylactic antibiotics in renal transplant recipients[J]. J Med Postgrad, 2020, 33(11): 1181-1186. DOI: 10.16571/j.cnki.1008-8199.2020.11.012. [19] 姜雪, 许书添, 顾鹏, 等. 肾移植受者感染的流行病学特点和危险因素[J]. 肾脏病与透析肾移植杂志, 2019, 28(6): 501-506. DOI: 10.3969/j.issn.1006-298X.2019.06.001.JIANG X, XU ST, GU P, et al. Epidemiology and risk factors of infections in kidney transplant recipients[J]. Chin J Nephrol Dial Transplant, 2019, 28(6): 501-506. DOI: 10.3969/j.issn.1006-298X.2019.06.001. [20] KUPELI E, ER DEDEKARGINOGLU B, ULUBAY G, et al. American Society of Anesthesiologists Classification versus ARISCAT risk index: predicting pulmonary complications following renal transplant[J]. Exp Clin Transplant, 2017, 15(Suppl 1): 208-213. DOI: 10.6002/ect.mesot2016.P89. [21] STRZELAK A, RATAJCZAK A, ADAMIEC A, et al. Tobacco smoke induces and alters immune responses in the lung triggering inflammation, allergy, asthma and other lung diseases: a mechanistic review[J]. Int J Environ Res Public Health, 2018, 15(5): 1033. DOI: 10.3390/ijerph15051033. [22] PEIFFER G, UNDERNER M, PERRIOT J. The respiratory effects of smoking[J]. Rev Pneumol Clin, 2018, 74(3): 133-144. DOI: 10.1016/j.pneumo.2018.04.009. [23] WAN H, WANG Y, FANG S, et al. Associations between the neutrophil-to-lymphocyte ratio and diabetic complications in adults with diabetes: a cross-sectional study[J]. J Diabetes Res, 2020: 6219545. DOI: 10.1155/2020/6219545. [24] 谭守勇, 袁园, 邝浩斌, 等. 中性粒细胞/淋巴细胞比值与2型糖尿病并发肺结核患者继发肺部感染相关性[J]. 中国防痨杂志, 2021, 43(6): 602-605. DOI: 10.3969/j.issn.1000-6621.2021.06.014.TAN SY, YUAN Y, KUANG HB, et al. Correlation between neutrophil-to-lymphocyte ratio and the secondary pulmonary infection in type 2 diabetes mellitus complicated with pulmonary tuberculosis[J]. Chin J Antitubercul, 2021, 43(6): 602-605. DOI: 10.3969/j.issn.1000-6621.2021.06.014. [25] NYUMURA I, HONDA K, BABAZONO T, et al. Recurrence of diabetic kidney disease in a type 1 diabetic patient after kidney transplantation[J]. Nephrology (Carlton), 2015, 20(Suppl 2): 90-92. DOI: 10.1111/nep.12454. [26] AKATA K, VAN EEDEN SF. Lung macrophage functional properties in chronic obstructive pulmonary disease[J]. Int J Mol Sci, 2020, 21(3): 853. DOI: 10.3390/ijms21030853. [27] SCHAUWVLIEGHE AFAD, RIJNDERS BJA, PHILIPS N, et al. Invasive aspergillosis in patients admitted to the intensive care unit with severe influenza: a retrospective cohort study[J]. Lancet Respir Med, 2018, 6(10): 782-792. DOI: 10.1016/S2213-2600(18)30274-1. [28] WIEDERMANN CJ. Hypoalbuminemia as surrogate and culprit of infections[J]. Int J Mol Sci, 2021, 22(9): 4496. DOI: 10.3390/ijms22094496. [29] ASTAPENKO D, BENES J, POUSKA J, et al. Endothelial glycocalyx in acute care surgery - what anaesthesiologists need to know for clinical practice[J]. BMC Anesthesiol, 2019, 19(1): 238. DOI: 10.1186/s12871-019-0896-2. [30] LABGAA I, JOLIAT GR, KEFLEYESUS A, et al. Is postoperative decrease of serum albumin an early predictor of complications after major abdominal surgery? a prospective cohort study in a European centre[J]. BMJ Open, 2017, 7(4): e013966. DOI: 10.1136/bmjopen-2016-013966. [31] LABGAA I, MANTZIARI S, GENETY M, et al. Early postoperative decrease of albumin is an independent predictor of major complications after oncological esophagectomy: a multicenter study[J]. J Surg Oncol, 2021, 123(2): 462-469. DOI: 10.1002/jso.26317. -

 下载:
下载:

 点击查看大图
点击查看大图
计量
- 文章访问数: 293
- HTML全文浏览量: 164
- PDF下载量: 85
- 被引次数: 0


