

-
摘要: 移植肝活组织检查(活检)病理学不仅在供肝病理学评估,而且在移植术后并发症的诊断和鉴别诊断中是不可缺少的。移植肝并发症的病理学诊断相关研究随着临床肝移植的扩展而日益深入,国际上逐渐制订了Banff移植肝活检病理学诊断标准,我国移植肝活检的病理学研究也逐步开展,并逐渐形成了适合我国肝移植临床实际的移植肝活检病理学诊断标准。本文对Banff移植肝活检病理学研究的历史和移植肝并发症的主要病变进行综述,旨在为我国更好地开展移植肝活检病理学诊断,协助临床进行肝移植术后并发症的明确诊断和针对性治疗,进一步提高移植肝和受者的良好存活提供参考依据。
-
关键词:
- 移植病理学 /
- 肝移植 /
- 活组织检查 /
- 病理学诊断标准 /
- 抗体介导的排斥反应(AMR) /
- T细胞介导的排斥反应(TCMR) /
- 慢性移植物血管病 /
- 药物性肝损伤
Abstract: The pathology of liver allograft biopsy is not only essential for the evaluation of liver donor, but also for the diagnosis and differential diagnosis of posttransplantation complications. With the development of liver transplantation in clinical practice, relevant studies of the pathological diagnosis of liver allograft complications have been deepened. Banff classification on liver allograft pathology have been gradually established within the international community. In China, pathological studies related to liver allograft pathology have been steadily carried out, and the pathological diagnostic basis of liver allograft pathology suitable for the clinical practice of liver transplantation in China has been gradually formed. This article reviews the history of Banff liver allograft pathology and major pathological lesions of liver allograft complications, aiming to provide reference for implementing pathological diagnosis of liver allograft pathology in China, assisting clinical diagnosis and targeted treatment of complications after liver transplantation, and further improving the survival of liver allograft and recipients. -

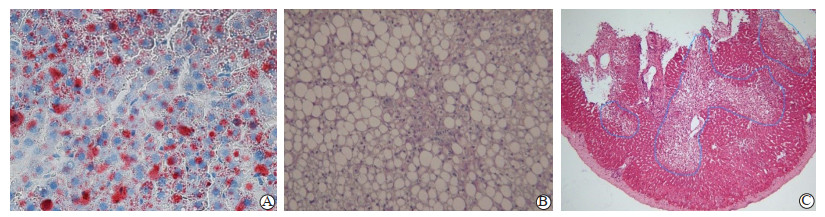
图 1 供肝大泡性脂肪变性和局灶性缺血性坏死的病理学表现
注:A图示供肝活检组织冷冻切片(油红O,×400),肝细胞内脂滴呈大颗粒红染阳性;B图示供肝活检快速石蜡切片中大多数肝细胞(>70%)明显大泡性脂肪变性(HE,×200);C图示供肝楔形活检组织内肝小叶腺泡Ⅲ区肝细胞缺血性坏死及部分区域两个肝小叶内坏死区域融合,蓝线内坏死肝细胞比例 > 20%(HE,×100)。
Figure 1. Pathological findings of macrovesicular steatosis and focal ischemic necrosis of the donor liver

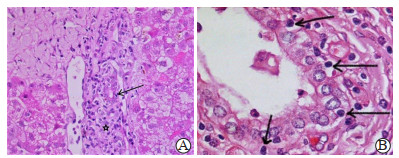
图 2 移植肝急性TCMR的病理学表现
注:A图示移植肝门管区内炎症细胞浸润,门管区内淋巴细胞浸润(星号所示)即小叶间胆管炎(箭头所示)(HE,×200);B图示门管区内小叶间胆管炎,可见小叶间胆管上皮内多个淋巴细胞浸润(箭头所示)(HE,×1 000)。
Figure 2. Pathological findings of acute TCMR in liver allograft

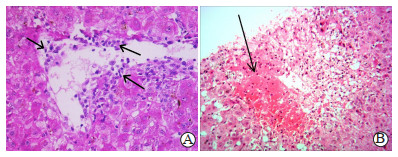
图 3 移植肝中央静脉炎型急性排斥反应的病理学表现
注:A图示中央静脉内皮炎表现(箭头所示)(HE,×400);B图示中央静脉周围肝细胞出血坏死(箭头所示)(HE,×200)。
Figure 3. Pathological findings of acute rejection of central venulitis in liver allograft

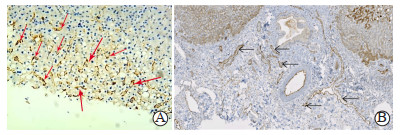
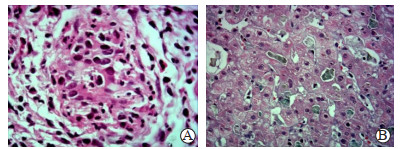
图 4 移植肝急性AMR的病理学表现
注:A图示部分肝窦内皮呈C4d阳性(箭头所示)(免疫酶组化,×200);B图示门管区内毛细血管内皮C4d阳性(箭头所示)(免疫酶组化,×200)。
Figure 4. Pathological findings of acute AMR in liver allograft

图 5 移植肝慢性排斥反应的病理学表现
注:A图示移植肝小叶间胆管萎缩及消失改变(HE,×400);B图示移植肝活检组织内CK19免疫组化染色(免疫酶组化,×400),可见小叶间胆管萎缩(箭头所示);C图示移植肝动脉的慢性排斥反应动脉血管病,图示肝动脉分支内膜泡沫细胞增生填塞及管腔狭窄(箭头所示)(HE,×400)。
Figure 5. Pathological findings of chronic rejection in liver allograft

图 6 移植肝胆管并发症的病理学表现
注:A图示移植肝活检组织门管区内轻微水肿,小叶间胆管周围及其上皮层内中性粒细胞浸润(HE,×400);B图示移植肝小叶中央区域内的毛细胆管明显扩张及胆汁淤积(HE,×400)。
Figure 6. Pathological findings of biliary complications in liver allograft

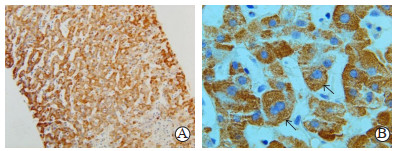
图 7 移植肝复发性乙型病毒性肝炎的病理学表现
注:A图示移植肝活检组织内HBsAg免疫组化染色在肝细胞呈弥漫性阳性(免疫酶组化,×200);B图示肝细胞胞浆内呈HBsAg阳性的病毒颗粒(箭头所示)(免疫酶组化,×1 000)。
Figure 7. Pathological findings of recurrent hepatitis B in liver allograft

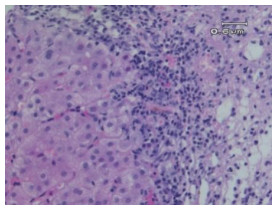
图 8 移植肝复发性自身免疫性肝炎病理学表现
注:图示移植肝活检组织内门管区周边典型的界板性炎症表现,同时可见局部的炎症向周围邻近肝组织扩展(HE,×200)。
Figure 8. Pathological findings of recurrent autoimmune hepatitis in liver allograft

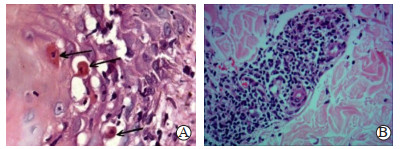
图 9 肝移植后GVHD所致皮疹的皮肤活检的病理学表现
注:A图示活检皮肤组织内鳞状上皮基底部有淋巴细胞及中性粒细胞浸润,基底细胞凋亡坏死呈“木乃伊细胞”(箭头所示)(HE,×400);B图示皮肤活检真皮组织内的微血管周围淋巴细胞围管状浸润(HE,×200)。
Figure 9. Pathological findings of skin biopsy of skin rash caused by GVHD after liver transplsntation
表 1 Banff标准中移植肝排斥反应的RAI评分
Table 1. RAI scoring of rejection of liver allograft in Banff classification
计分(分) 门管区炎症 胆管炎症 血管炎症 1 仅少数的门管区内可见淋巴细胞等炎症细胞浸润,门管区范围无明显扩大 少数小叶间胆管上皮内炎症细胞浸润和胆管上皮轻度损伤改变(包括细胞核增大、核/浆比增加) 少数小叶间血管(小叶间动脉或小叶间静脉)和(或)中央静脉的血管炎表现 2 多数或全部门管区内均出现混合性炎症细胞浸润(包括淋巴细胞、浆细胞、少数中性粒细胞和嗜酸性粒细胞等),门管区扩大。如果出现多量嗜酸性粒细胞浸润伴门管区水肿和微血管内皮细胞肿大改变,应注意急性AMR因素 多数胆管上皮内炎症细胞浸润,较多胆管出现损伤改变包括胞核多形性、极像紊乱和胞浆空泡变 多数或全部小叶间血管和(或)中央静脉的血管炎表现,少数中央静脉周围肝细胞脱失 3 多数或全部门管区出现混合性炎症细胞浸润,门管区因水肿和大量炎症细胞浸润范围扩大,部分门管区内炎症细胞扩展进入周围肝组织内 在2的基础上出现多数或全部胆管退化或灶性胆管腔破坏崩解 在2的基础上,出现中重度中央静脉炎及其周围炎并延伸至周围肝实质和中央静脉周围多数肝细胞坏死  下载: 导出CSV
下载: 导出CSV
表 2 移植肝慢性排斥反应的病理学诊断标准
Table 2. Pathological diagnostic criteria for chronic rejection of liver allograft
主要病变部位 早期的慢性排斥反应
(至少符合两条)晚期的慢性排斥反应
(至少符合两条)小胆管(< 60 μm) 多数门管区内小叶间胆管出现损伤, < 50%门管区出现小叶间胆管消失 ≥50%门管区出现小叶间胆管消失,其余门管区内小叶间胆管出现损伤退化 小叶间动脉 < 25%门管区出现小叶间动脉消失 ≥25%门管区出现小叶间动脉消失 终末肝静脉和Ⅲ区肝细胞 终末肝静脉周围单个核细胞浸润,腺泡Ⅲ区肝细胞坏死和炎症细胞浸润,轻度纤维化 终末肝静脉程度不等的炎症细胞浸润,局灶性静脉闭塞,中到重度(桥样)纤维化 肝动脉主干分支 动脉内膜炎、局灶性泡沫细胞沉积,无管腔狭窄或闭塞 内膜泡沫细胞沉积及纤维组织增生导致管腔狭窄甚至闭塞 胆管主干分支 炎症损伤和灶性泡沫细胞沉积 管壁纤维化 其他 “过渡性”肝炎和多灶性肝细胞坏死 肝窦泡沫细胞沉积、胆汁淤积
下载: 导出CSV
-
[1] Banff schema for grading liver allograft rejection: an international consensus document[J]. Hepatology, 1997, 25(3): 658-663. DOI: 10.1002/hep.510250328. [2] DEMETRIS A, ADAMS D, BELLAMY C, et al. Update of the International Banff Schema for liver allograft rejection: working recommendations for the histopathologic staging and reporting of chronic rejection. an international panel[J]. Hepatology, 2000, 31(3): 792-799. DOI: 10.1002/hep.510310337. [3] 郭晖. 移植肾抗体介导的排斥反应的病理学[J]. 器官移植, 2021, 12(3): 262-271. DOI: 10.3969/j.issn.1674-7445.2021.03.003.GUO H. Pathology of antibody-mediated rejection in renal allograft[J]. Organ Transplant, 2021, 12(3): 262-271. DOI: 10.3969/j.issn.1674-7445.2021.03.003. [4] MENGEL M, SIS B, HAAS M, et al. Banff 2011 meeting report: new concepts in antibody-mediated rejection[J]. Am J Transplant, 2012, 12(3): 563-570. DOI: 10.1111/j.1600-6143.2011.03926.x. [5] HAAS M, SIS B, RACUSEN LC, et al. Banff 2013 meeting report: inclusion of C4d-negative antibody-mediated rejection and antibody-associated arterial lesions[J]. Am J Transplant, 2014, 14(2): 272-283. DOI: 10.1111/ajt.12590. [6] DEMETRIS AJ, BELLAMY C, HÜBSCHER SG, et al. 2016 Comprehensive update of the Banff Working Group on liver allograft pathology: introduction of antibody-mediated rejection[J]. Am J Transplant, 2016, 16(10): 2816-2835. DOI: 10.1111/ajt.13909. [7] 中华医学会器官移植学分会, 中国医师协会器官移植医师分会, 中国抗癌协会肝癌专业委员会病理学组, 等. 肝移植常见并发症病理诊断指南(2016版)[J]. 中华器官移植杂志, 2016, 37(8): 494-501. DOI: 10.3760/cma.j.issn.0254-1785.2016.08.010.Branch of Organ Transplantation of Chinese Medical Association, Branch of Organ Transplant Physician of Chinese Medical Doctor Association, Pathological Group of Chinese Society of Liver Cancer of Chinese Anti-cancer Association, et al. Guideline for the pathological diagnosis of common complications after liver transplantation (2016 edition)[J]. Chin J Organ Transplant, 2016, 37(8): 494-501. DOI:10.3760/cma.j.issn. 0254-1785.2016.08.010. [8] 中华医学会器官移植学分会. 器官移植病理学临床技术操作规范(2019版)——肝移植[J]. 器官移植, 2019, 10(3): 267-277. DOI: 10.3969/j.issn.1674-7445.2019.03.008.Branch of Organ Transplantation of Chinese Medical Association. Clinical technical operation specification for pathology of organ transplantation (2019 edition): liver transplantation[J]. Organ Transplant, 2019, 10(3): 267-277. DOI: 10.3969/j.issn.1674-7445.2019.03.008. [9] JIMÉNEZ-CASTRO MB, CASILLAS-RAMÍREZ A, NEGRETE-SÁNCHEZ E, et al. Adipocytokines in steatotic liver surgery/transplantation[J]. Transplantation, 2019, 103(1): 71-77. DOI: 10.1097/TP.0000000000002098. [10] ÁLVAREZ-MERCADO AI, GULFO J, ROMERO GÓMEZ M, et al. Use of steatotic grafts in liver transplantation: current status[J]. Liver Transpl, 2019, 25(5): 771-786. DOI: 10.1002/lt.25430. [11] BABA HA, THEURER S, CANBAY A, et al. Liver transplantation. current aspects of pretransplantation diagnosis and rejection[J]. Pathologe, 2020, 41(5): 505-514. DOI: 10.1007/s00292-020-00813-9. [12] KOO J, WANG HL. Acute, chronic, and humoral rejection: pathologic features under current immunosuppressive regimes[J]. Surg Pathol Clin, 2018, 11(2): 431-452. DOI: 10.1016/j.path.2018.02.011. [13] KIM PT, DEMETRIS AJ, O'LEARY JG. Prevention and treatment of liver allograft antibody-mediated rejection and the role of the 'two-hit hypothesis'[J]. Curr Opin Organ Transplant, 2016, 21(2): 209-218. DOI: 10.1097/MOT.0000000000000275. [14] MILLER CM, DURAND F, HEIMBACH JK, et al. The international liver transplant society guideline on living liver donation[J]. Transplantation, 2016, 100(6): 1238-1243. DOI: 10.1097/TP.0000000000001247. [15] O'LEARY JG, CAI J, FREEMAN R, et al. Proposed diagnostic criteria for chronic antibody-mediated rejection in liver allografts[J]. Am J Transplant, 2016, 16(2): 603-614. DOI: 10.1111/ajt.13476. [16] KOZLOWSKI T, ANDREONI K, SCHMITZ J, et al. Sinusoidal C4d deposits in liver allografts indicate an antibody-mediated response: diagnostic considerations in the evaluation of liver allografts[J]. Liver Transpl, 2012, 18(6): 641-658. DOI: 10.1002/lt.23403. [17] ALI S, ORMSBY A, SHAH V, et al. Significance of complement split product C4d in ABO-compatible liver allograft: diagnosing utility in acute antibody mediated rejection[J]. Transpl Immunol, 2012, 26(1): 62-69. DOI: 10.1016/j.trim.2011.08.005. [18] BOEVA I, KARAGYOZOV PI, TISHKOV I. Post-liver transplant biliary complications: current knowledge and therapeutic advances[J]. World J Hepatol, 2021, 13(1): 66-79. DOI: 10.4254/wjh.v13.i1.66. [19] MAGRO B, TACELLI M, MAZZOLA A, et al. Biliary complications after liver transplantation: current perspectives and future strategies[J]. Hepatobiliary Surg Nutr, 2021, 10(1): 76-92. DOI: 10.21037/hbsn.2019.09.01. [20] GERMANI G, BATTISTELLA S, ULINICI D, et al. Drug induced liver injury: from pathogenesis to liver transplantation[J]. Minerva Gastroenterol (Torino), 2021, 67(1): 50-64. DOI: 10.23736/S1121-421X.20.02795-6. [21] DEVARBHAVI H, AITHAL G, TREEPRASERTSUK S, et al. Drug-induced liver injury: Asia Pacific Association of Study of Liver consensus guidelines[J]. Hepatol Int, 2021, 15(2): 258-282. DOI: 10.1007/s12072-021-10144-3. [22] JIMÉNEZ-PÉREZ M, GONZÁLEZ-GRANDE R, GARCÍA-CORTÉS M, et al. Drug-induced liver injuryafter liver transplantation[J]. Liver Transpl, 2020, 26(9): 1167-1176. DOI: 10.1002/lt.25804. [23] 中华医学会感染病学分会, 中华医学会肝病学分会. 慢性乙型肝炎防治指南(2019年版)[J/CD]. 中国肝脏病杂志(电子版), 2019, 11(4): 5-27. DOI: 10.3969/j.issn.1674-7380.2019.04.002.Branch of Infectious Diseases of Chinese Medical Association, Branch of Hepatology of Chinese Medical Association. The guideline of prevention and treatment for chronic hepatitis B: a 2019 update[J/CD]. Chin J Liver Dis(Electr Vers), 2019, 11(4): 5-27. DOI: 10.3969/j.issn.1674-7380.2019.04.002. [24] WANG Q, HUANG A, WANG JB, et al. Chronic drug-induced liver injury: updates and future challenges[J]. Front Pharmacol, 2021, 12: 627133. DOI: 10.3389/fphar.2021.627133. [25] KERKAR N, YANNI G. 'De novo' and 'recurrent' autoimmune hepatitis after liver transplantation: a comprehensive review[J]. J Autoimmun, 2016, 66: 17-24. DOI: 10.1016/j.jaut.2015.08.017. [26] BEER A, DIENES HP. Autoimmune hepatitis-is histology conclusive?[J]. Ann Transl Med, 2021, 9(8): 733. DOI: 10.21037/atm-20-5084. [27] MIYAGAWA-HAYASHINO A, HAGA H, EGAWA H, et al. Idiopathic post-transplantation hepatitis following living donor liver transplantation, and significance of autoantibody titre for outcome[J]. Transpl Int, 2009, 22(3): 303-312. DOI: 10.1111/j.1432-2277.2008.00803.x. [28] SWERDLOW SH, CAMPO E, PILERI SA, et al. The 2016 revision of the World Health Organization classification of lymphoid neoplasms[J]. Blood, 2016, 127(20): 2375-2390. DOI: 10.1182/blood-2016-01-643569. -

 下载:
下载:


 点击查看大图
点击查看大图

计量
- 文章访问数: 1477
- HTML全文浏览量: 540
- PDF下载量: 306
- 被引次数: 0


